The NPs' dirty laundry, round 2: Reaction to diploma mills
💬 0 comments
In reference to Round 1 for PMHNPs



An article entitled "Boosting Profits Drives NP Diploma Mills" published in the February 2021 issue of Emergency Medicine News has been making quite a few waves, among both physicians and midlevels alike. The article provides an excellent overview of the ever-sinking bar for admission into nurse practitioner degree-granting programs, with some specific examples of large programs that had a 100% admission rate for the hundreds of applicants that applied. At this rate, programs might as well be advertising the minimum GCS score applicants need to be admitted. Here, we compile some of the NP community's colorful reactions to this article.
House built on sand
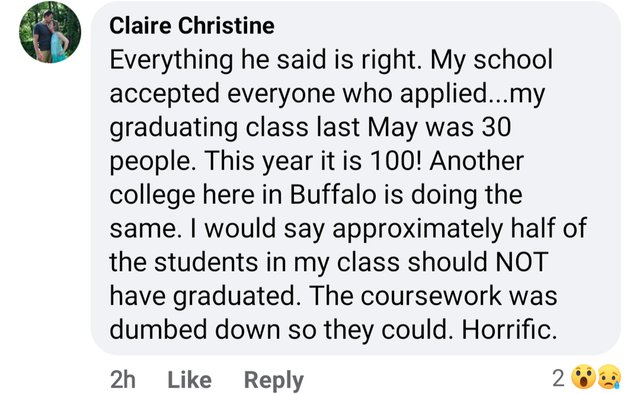
This nurse practitioner appears to have graduated from the D'Youville University PMHNP program, which, interestingly, is a brick-and-mortar program with classes held on Tuesday and Thursdays. However, it only requires a minimum GPA of 3.0 (or as low as 2.7 for nurses with degrees earned >5 years ago "who have achieved significant professional success", whatever that means), and a "writing assignment on your philosophy of nursing, 2 pages in length, double space and 12-point font". No standardized entrance exam required! Clearly, it's not just the online, for-profit diploma mills that are part of the problem.
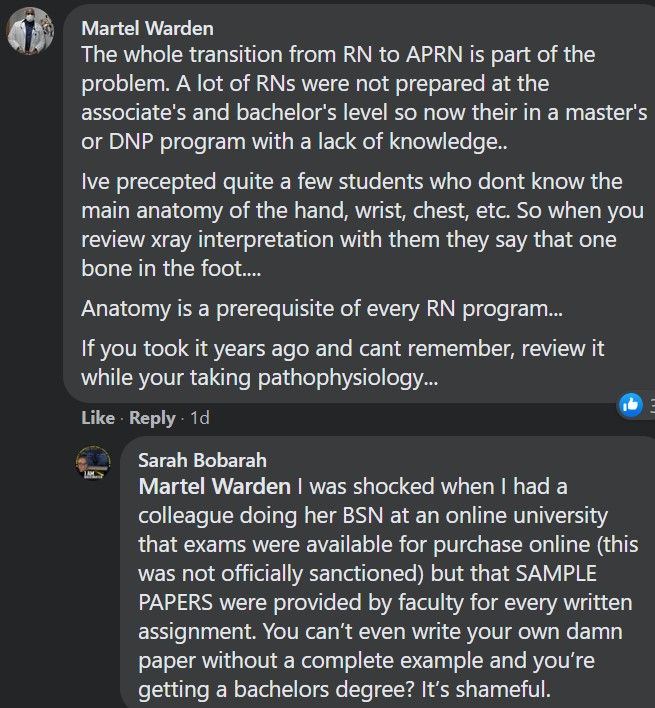
Wow. Can you imagine a medical student passing pre-clinicals if they flunked basic anatomy this hard? Hell, many medical schools won't even allow their students to progress to M2 year without a passing grade in anatomy. It's safe to say that if you're a medical student, not being able to identify the basic anatomy of the hand, wrist, or chest is a good sign that your career in medicine is going to be a short-lived failure. Not so for nursing, apparently. You can keep on going, all the way until you become a Doctor of Nursing Practice! There's nothing that screams "terminal degree-holder" like not being able to identify bones on an X-ray. Remember, these are the same group of folks who clamor for full independent practice rights while calling themselves "Doctor" and proclaiming equivalence (and even superiority) to physicians.
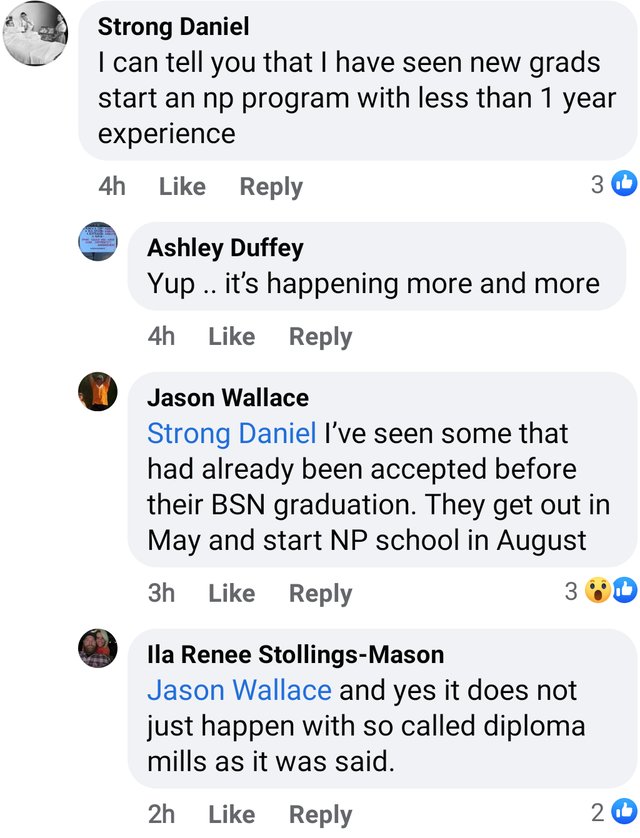

It gets even better, though. Why bother transitioning from an RN to an APRN/NP when you can just skip the RN step entirely? With the advent of direct-entry programs, you don't even need an undergraduate nursing degree to get an MSN or DNP. Why bother with 4+ years of medical school, 3+ years of residency, and 1+ years of fellowship when it's this easy to become a pseudo-doctor?
Nursing ≠ Medicine
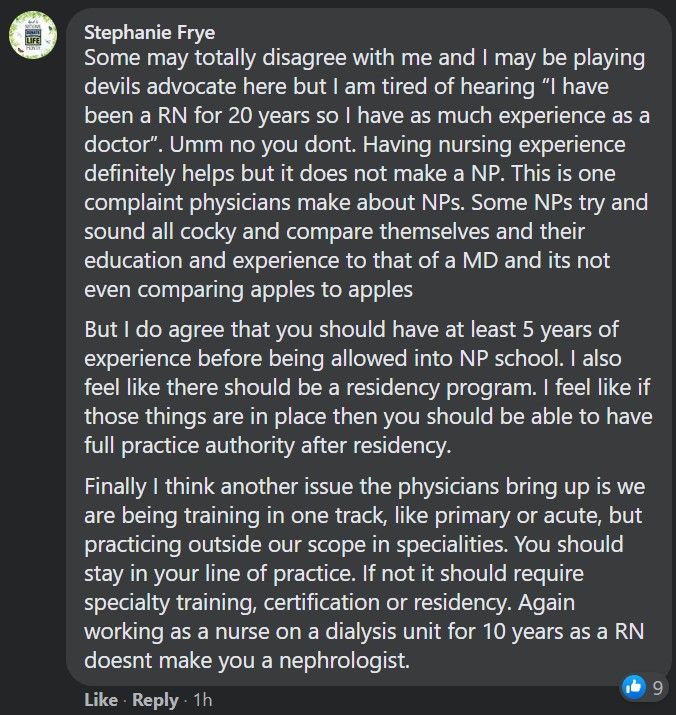
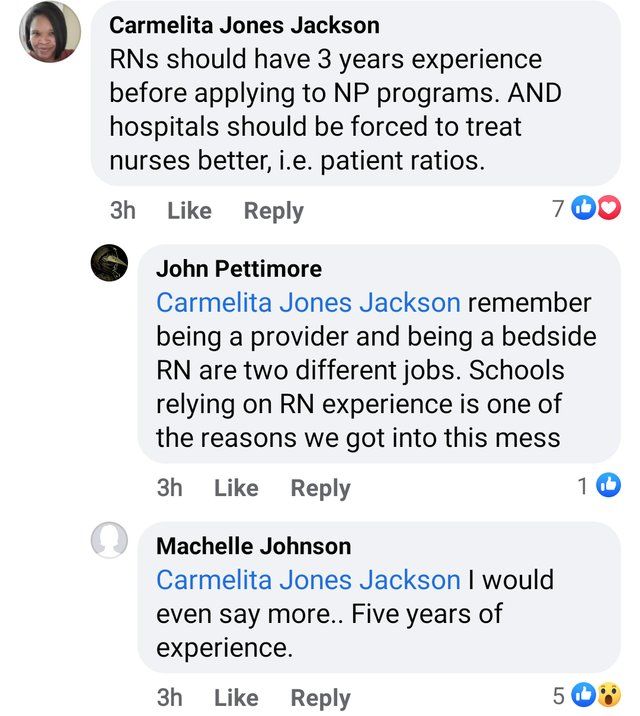
One Dunning-Kruger-esque argument that NPs love to make whenever their competence is questioned is "hurr durr, I've been a nurse for X years, so now that I'm a nurse practitioner I'm just as, if not more experienced than a physician!" Thankfully, not all NPs are blind to reality. At a fundamental level, nursing is not medicine. No ifs, thens, or buts about it. If years of nursing experience and completion of an NP degree program was truly equivalent to years of medical training, we would not see an NP with almost a decade of nursing experience have no idea how to handle a common and straightforward complaint like vaginal discharge.
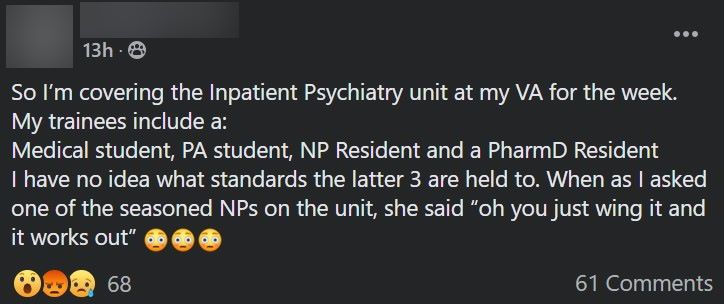
This might be due to the fact that NP programs typically include only 500-700 hours of clinical "training" - "training" being a relative term, given that many of these hours could amount to little more than shadowing. Or, in some cases, unsanctioned coffee breaks.
Clean Up Your Own Backyard
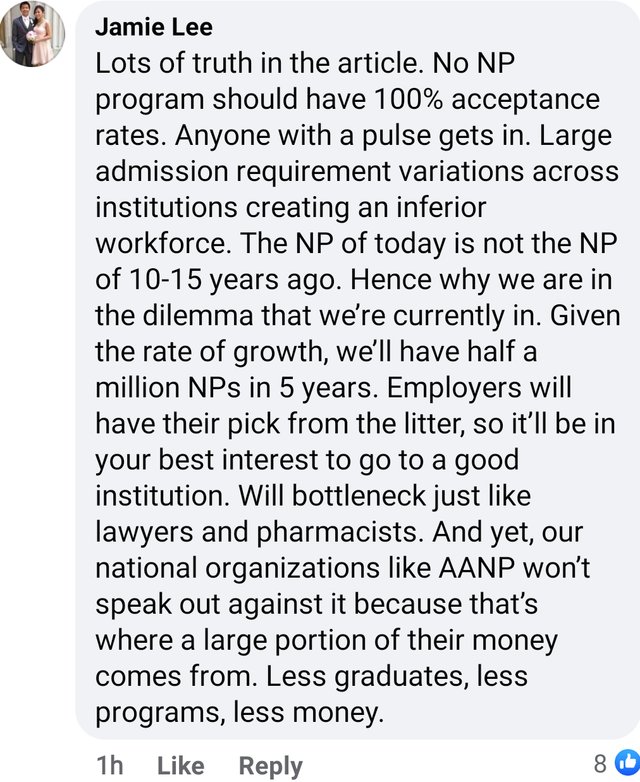
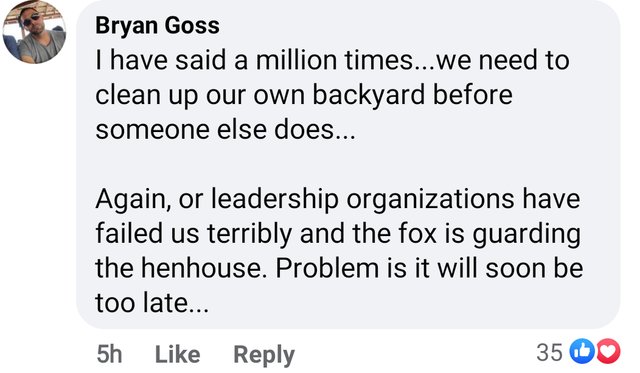
As these wise commenters have noted, the first step to addressing the gross inadequacy of nurse practitioner education and resulting clinical incompetence is for their national leadership organizations to start clamping down. Will that come in the form of more rigorous admissions requirements? Formal educational standards with uniform guidelines for clinical hours? Recommending nullification of independent practice statutes and reverting to a direct physician supervision model that midlevels were originally intended to operate under? Anything would be better than nothing, which is what the American Association of Nurse Practitioners (AANP)'s current position seems to be when it comes to diploma mills and granting NP degrees to warm bodies with wallets. Rather, the AANP seems to be more concerned with lobbying for Full Practice Authority in every state in the country.
Put in perspective, it's truly mind-boggling to envisage the sheer disparity between NPs' minimal education standards and the increasingly broad scope of practice and medical decision-making they are being given by legislatures and health systems. And unfortunately, with NPs being governed under nursing (instead of medical boards), there's little to no accountability when an inadequately-trained, inadequately-supervised nurse practitioner inevitably fucks up. This is a problem seemingly unique to the NP profession. For example, while medical school diploma mills certainly exist (usually in the Carribean), graduates of these programs must still possess the minimum degree of academic competence required to pass the USMLE exams, spend the same amount of time completing clinical rotations stateside, but for various reasons are punished heavily later on with low match rates into residency programs compared to graduates of reputable US MD/DO institutions. It turns out that residency and fellowship program directors, at least, have some semblance of minimum educational standards they try to uphold. While getting into an NP program seems to be becoming easier and easier by the day, successfully matching into residency only seems to get tougher. And certainly, we haven't heard of issues with nuclear engineers and police officers graduating from diploma mills. Say what you want about the state of law enforcement in this country, but it's certainly safe to say that the training and conduct of police officers these days is being scrutinized much more closely than that of nurse practitioners, even if the latter is just as capable of killing someone innocent through faulty medical decision-making and malpractice. Are these the kinds of healthcare practitioners we want to be entrusting our lives to? Until the NP profession decides to clean house and put patients before profits and ego, our answer is a resounding no.



