Urine trouble: NPs demonstrate a piss-poor understanding of pee
💬 0 comments
Urine for a real golden treat with this post.
You can tell when a midlevel is desperate for advice when they post their question to not one, but TWO Facebook groups. Today we have another golden example of a midlevel social media consult for our readers to enjoy while they're on the shitter, answering nature's call. Feast your eyes on the following posts from a family nurse practitioner by the name of Thuyan Nguyen:
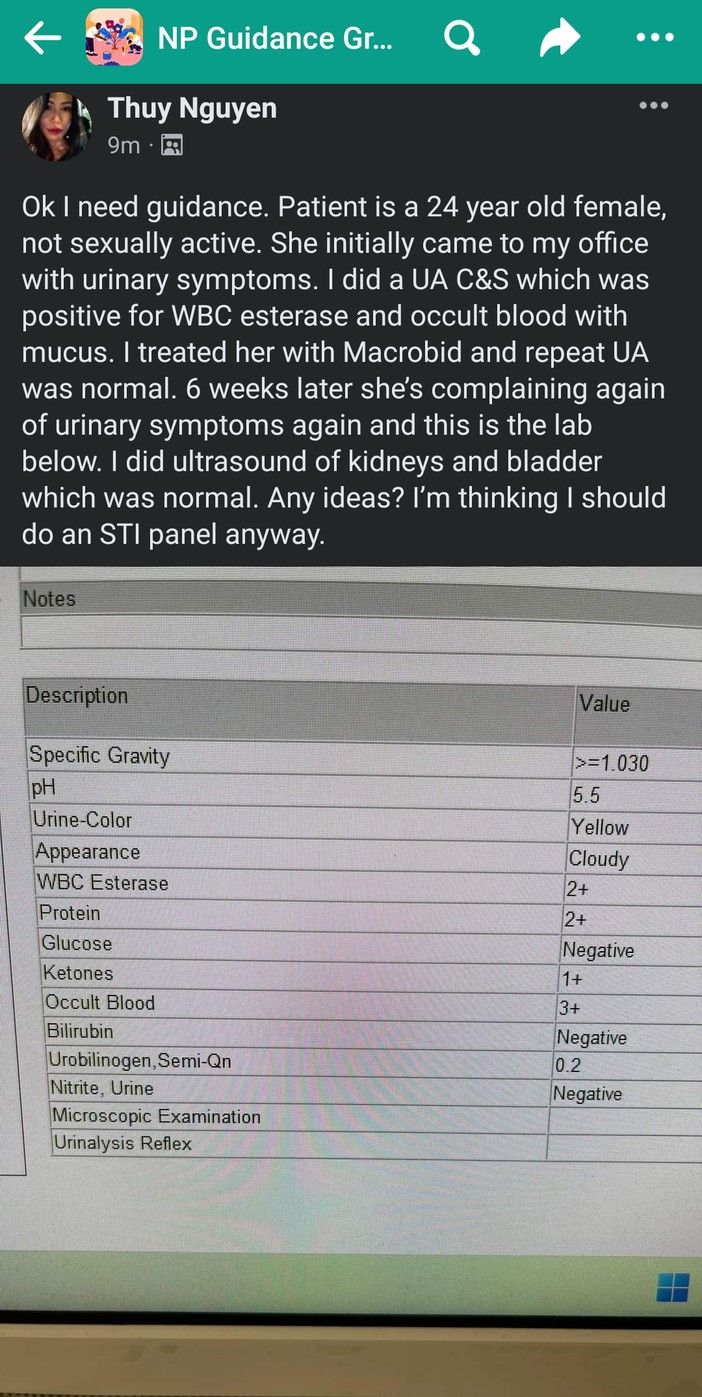
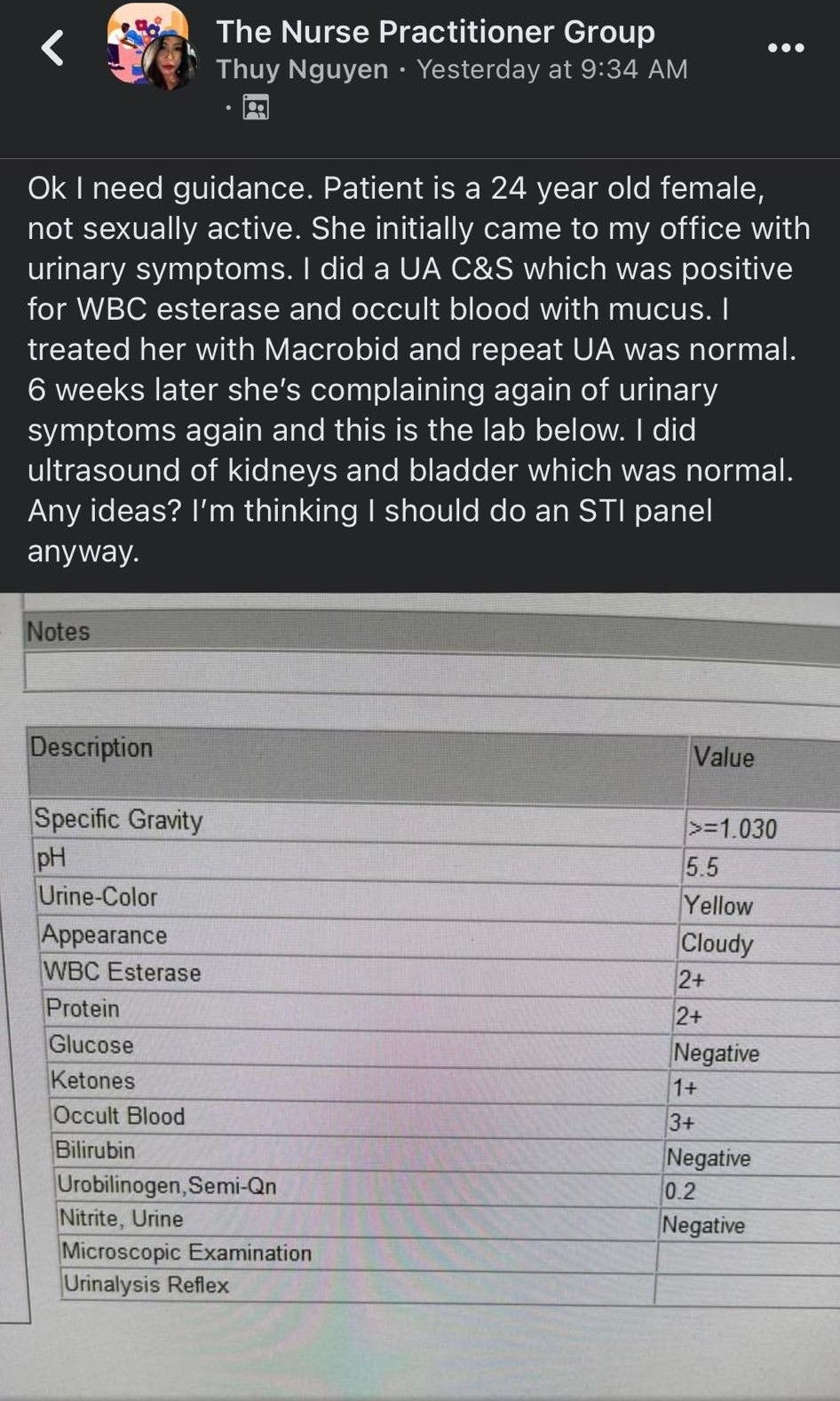
Here we have another classic example of how shoddy the typical midlevel consult is. "Urinary symptoms"? Can you be any more vague? Was there dysuria? Malodorous urine? Urinary frequency? Hesitancy? Gross hematuria? You can't just tell us that you did a urine culture and sensitivity and then provide absolutely no information on what the results of that were. Why Macrobid as opposed to any other antibiotic? What was the clinical reasoning to jump to ultrasounds of the kidneys and bladder? Why an STI panel if the patient is "not sexually active"? There are so many unanswered questions and unexplained medical decisions here.
But, as is often the case, the real midlevel comedy gold lies in the comments section. "The blind leading the blind" would be too charitable of a description, because quite frankly, some of the responses from other midlevel NPs are so utterly idiotic that they make us want to gouge our own eyes out. Let's look at a few of them.
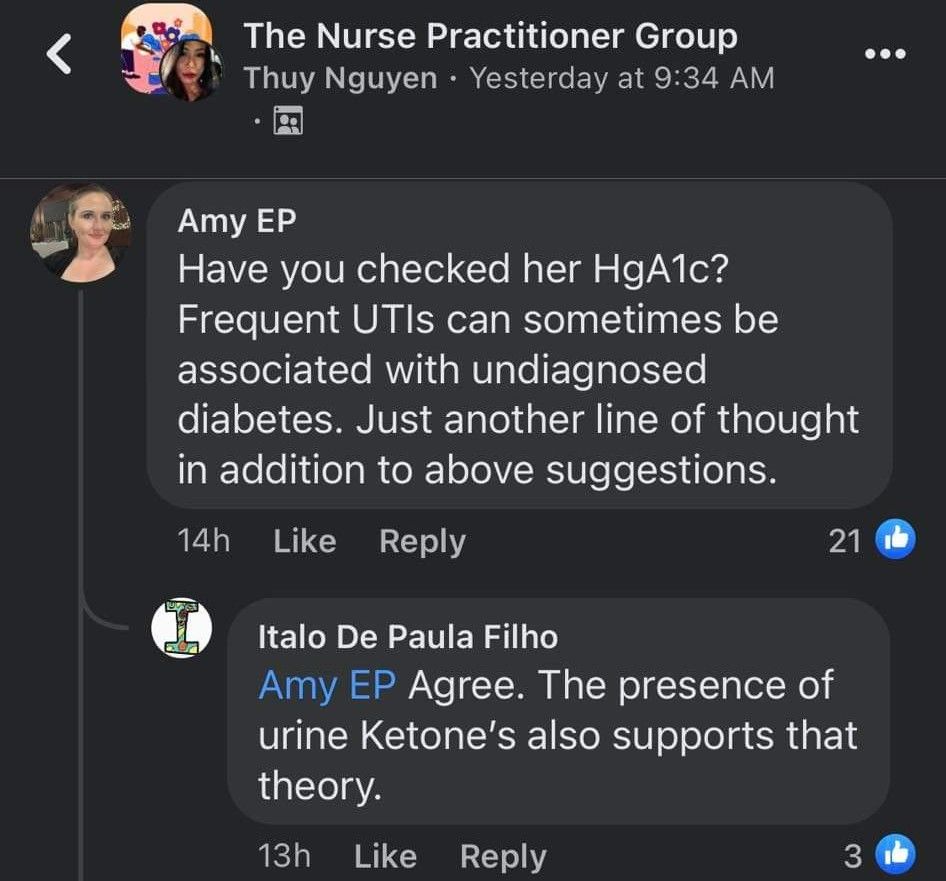
Did these twats completely neglect to appreciate the fact that the urinalysis is completely NEGATIVE for glucose? Are they aware that many things other than diabetes (e.g. dehydration) can cause ketones to be present in urine? Do they really think that 1+ ketones in urine, combined with the complete absence of glycosuria, could possibly be due to symptomatic, undiagnosed diabetes?
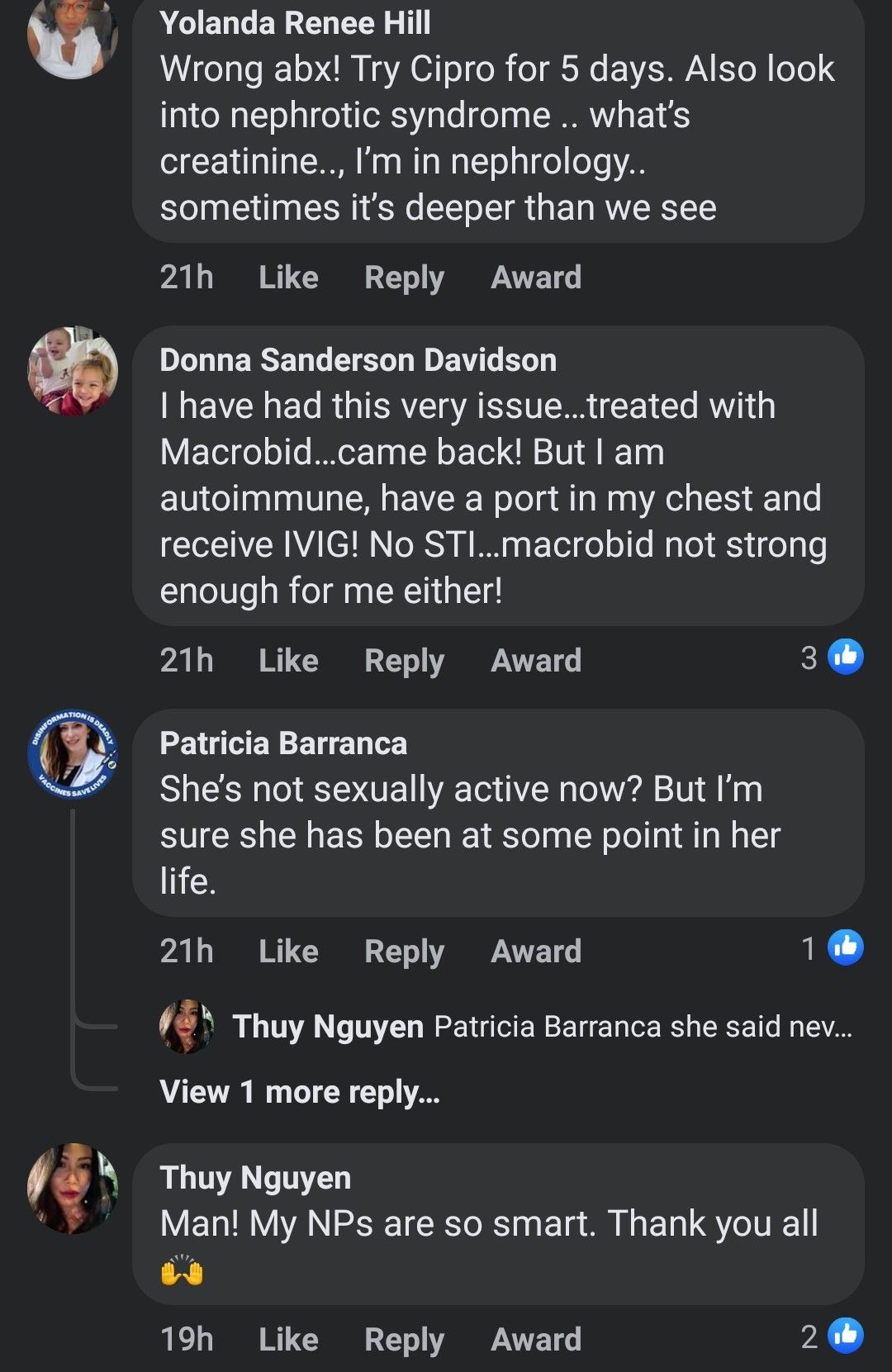
"My NPs are so smart?" On the contrary, if this thread is any indication, they are dumber than a bag of urine-soaked bricks. Gotta love NP Yolanda Hill's brazen suggestion to pull out the proverbial shotgun and jump straight to Cipro, when we don't even know for sure if this is a UTI and we have absolutely no fucking idea what the urine culture and sensitivities look like. It's painfully ironic that NP Yolanda is blindly suggesting Cipro yet claims to work in nephrology, given that Cipro has been linked to crystal-induced acute kidney injury.
And lest we forget about NP Patricia and her assumptions about the patient's sexual activity. Wow, presumptuous much?
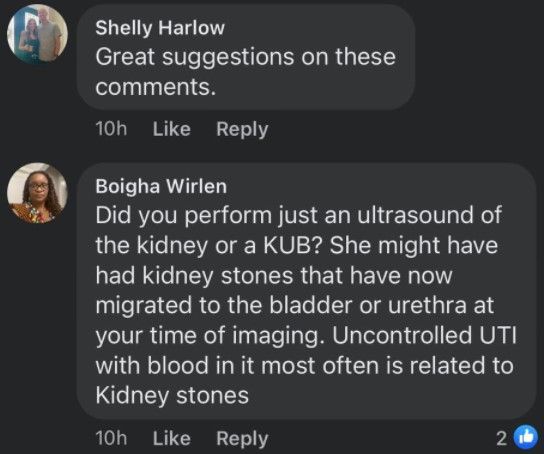
To continue with our theme of greatly terrible suggestions, now we have another NP by the name of Giselle Boigha Wirlen, who apparently owns an IV cocktail infusion joint in Texas, bringing up the highly questionable possibility of kidney stones. Lol wut? What are the chances of a kidney stone going away after treatment with Macrobid, then returning six weeks later with a negative renal ultrasound? And "uncontrolled UTI with blood in it most often is related to kidney stones"? What in the actual urological fuck? Sounds like someone's had a few too many of those $250 signature IV cocktails.
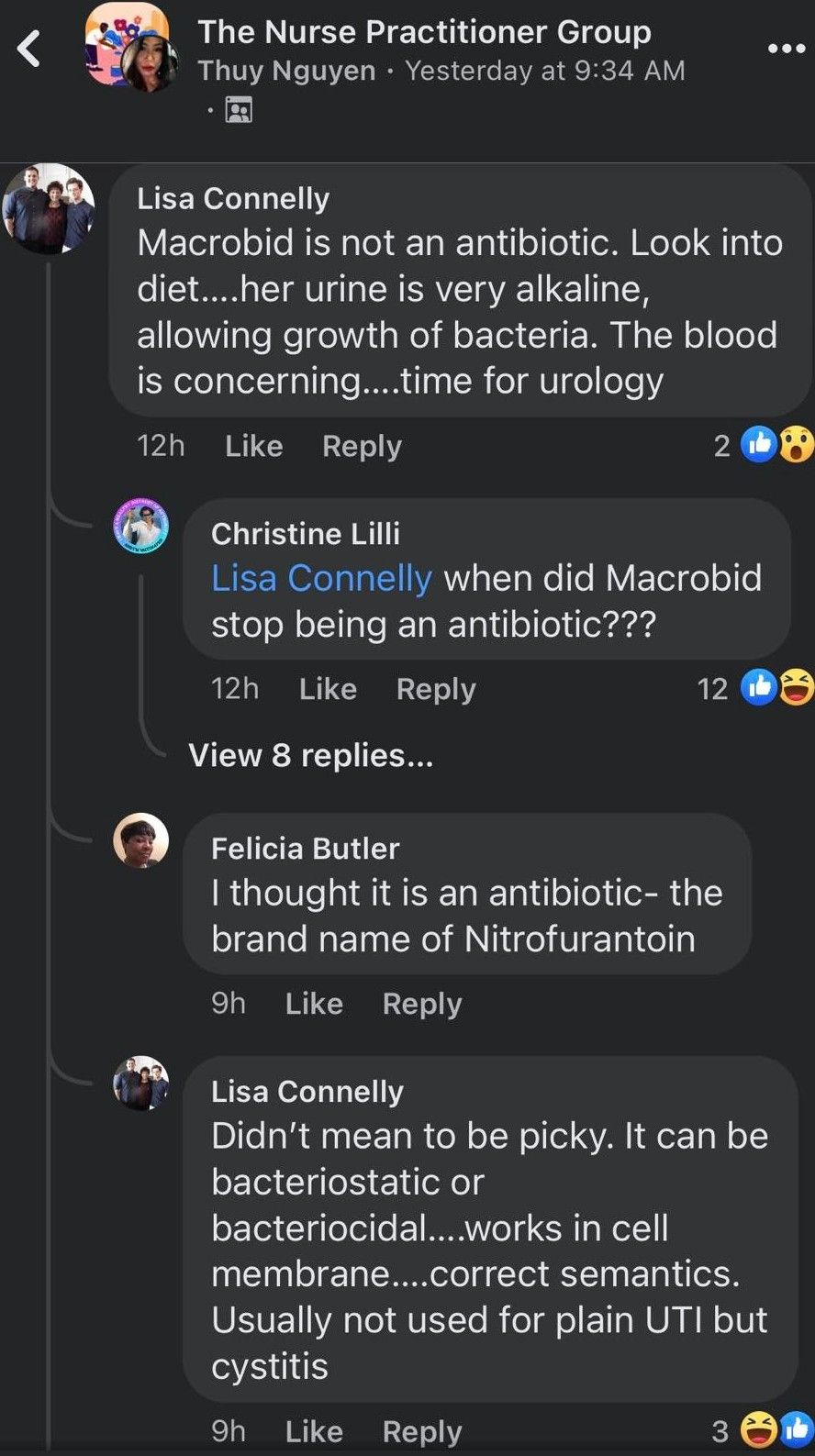
And last but certainly not least, we have FNP Lisa Connelly coming in hot with not one, but THREE golden shower-worthy proclamations!
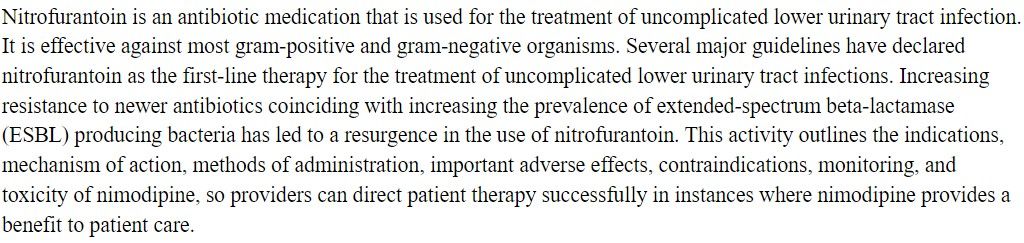
- "Macrobid is not an antibiotic" - What in the actual monohydrated fuck? It's truly horrific that politicians give midlevels like these the legal authority to write prescriptions, let alone have full practice authority.
- "Her urine is very alkaline" - for a urine sample with a pH of 5.5 (i.e. completely normal). Good lord, we don't need a urology consult, we need a high school chemistry textbook! In what universe is a pH of 5.5 considered alkaline?!
- Macrobid [is] "usually not used for plain UTI but cystitis"? Uhh, what? Literally every reputable medical reference would beg to differ.
Jesus fucking Christ, the combined stupidity of these blatantly false statements burns harder than an elderly woman with a UTI caught in a house fire.

This cross-section of midlevel NP Facebook commentary is not only an excellent reminder of why it's a piss-poor idea to use social media for clinical references, but also a glaring indictment of the turd-like state of nurse practitioner education in the 21st century. If you can't even work up a basic urinary complaint, you have absolutely no business being anywhere near a real patient.



