Tests, tests, and more tests
💬 0 comments
Shotgunning labs is not an acceptable substitute for clinical acumen and an understanding of pathophysiology.
The diagnostic acumen and clinical sixth sense that physicians develop after years and years of medical school, residency, and possibly fellowship is something that is all too underappreciated. Compared to physicians, midlevels order more tests, prescribe more drugs, place lower-quality consults, and are responsible for a higher share of diagnosis and treatment-related malpractice claims. Simply put, the training and experience of an attending physician cannot be replicated or approximated with a nurse practitioner who graduated from a 100%-online, for-profit diploma mill with only 500-600 clinical "training" hours that might have amounted to little more than shadowing.
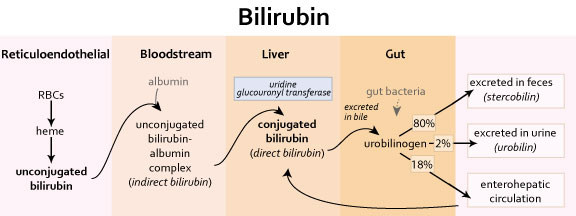
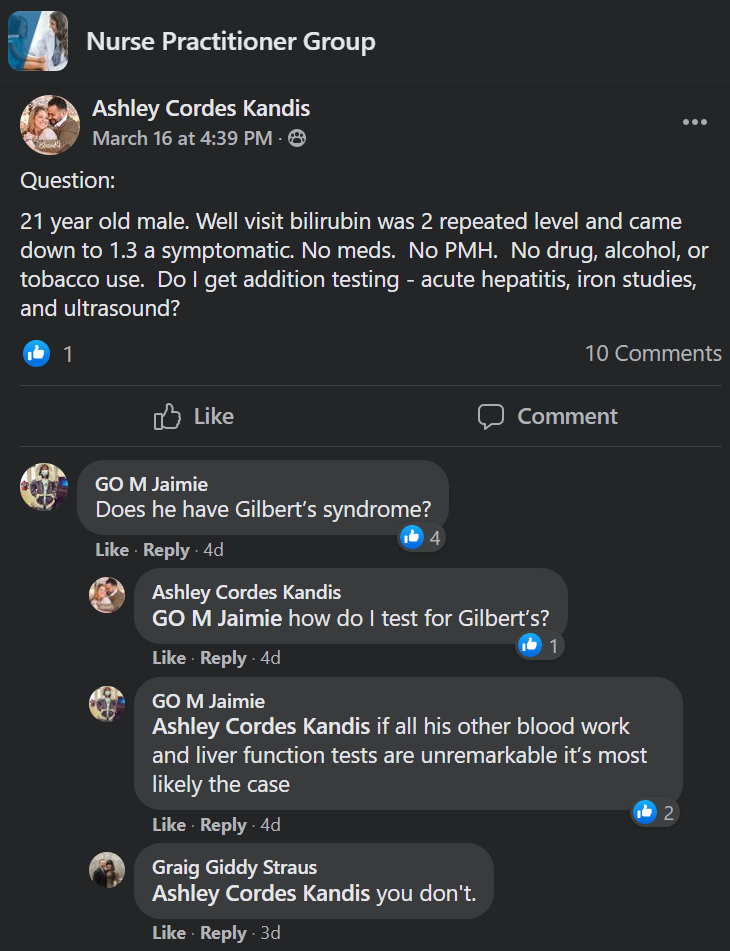
This post from an NP named Ashley Kandis is a perfect example. Here we have a 21-year-old male, seemingly otherwise healthy, presenting with asymptomatic hyperbilirubinemia. Does this NP know the basic underlying physiology of the bilirubin pathway? The pathophysiology of common conditions that can cause elevations in direct or indirect bilirubin? Do they even teach these things in nurse practitioner school? Evidently not, when the kneejerk reflex is to start rattling off additional laboratory tests to order. At least the comment section seems to possess a little more clinical intelligence - Gilbert's syndrome is a likely suspect in an asymptomatic young person.
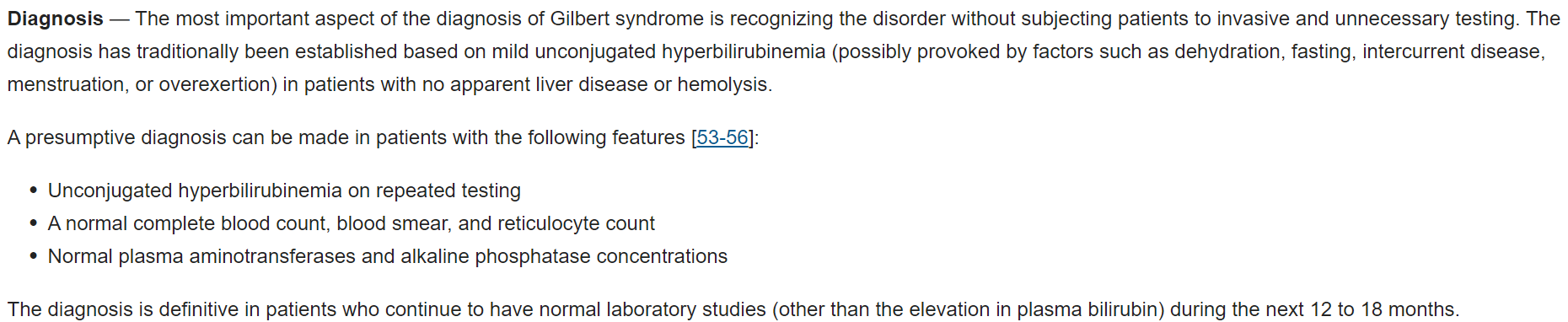
Of course, basic metabolic pathways and their associated pathologies are concepts that every successful first- and second-year medical student have drilled into their brains. It's standard fare on the USMLE Step 1 exam. One would be hard-pressed to find a medical student who didn't know what Gilbert's syndrome was and that it's not something that typically requires additional laboratory testing. Whereas a nurse practitioner (like this one) asks, "How do I test for Gilbert's?" (do they even know what Gilbert's syndrome is?), a physician would have the common sense to know that you basically don't specifically test for it. This is where physicians show their mettle; physicians are able to use their education and training in conjunction with their critical thinking skills to formulate a differential diagnosis, confirm their suspicions with appropriate, relevant, and clinically justifiable lab tests, and differentiate between benign and serious conditions. By contrast, midlevels tend to shotgun labs and come up with a diagnosis after the fact to see what sticks. Needless to say, this is an inefficient, expensive (especially for the patient), and clinically painful way of practicing medicine!



