Strep throat antibiotic roulette
💬 0 comments
We developed antibiotic-induced Clostridium difficile infection after reading this post.
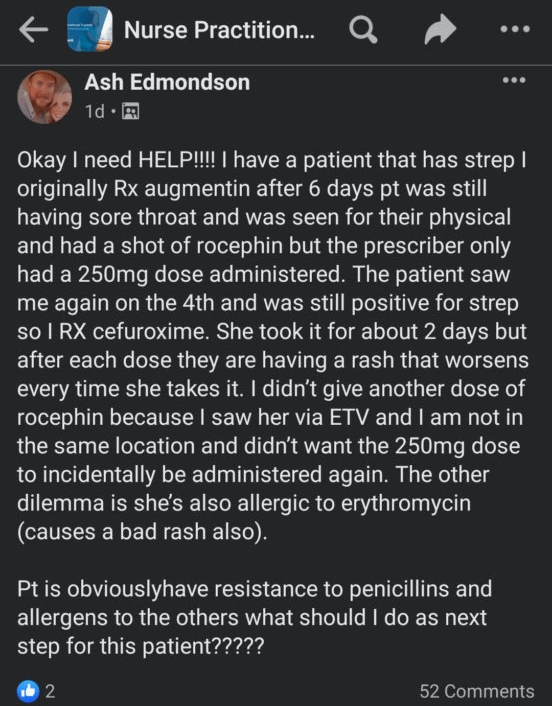
OMG!!!! Can someone help this perplexed nurse practitioner????? Augmentin for six days, a shot of Rocephin, with cefuroxime for dessert...it's a miracle this patient didn't get a raging C. diff infection. There's so much to unpack here with FNP Ashley Edmondson's genius-level medical decision-making. Like, who treats strep throat right off the bat with Augmentin as the first line? What the hell is a single dose of IM Rocephin going to do, or even two? (As if "I saw her via ETV and I am not in the same location [as the patient]" is a remotely logical reason for not giving another dose of IM Rocephin). Why would cefuroxime work if the patient already received Rocephin, another cephalosporin? "Pt is obviously have resistance to penicillins and allergens to the others"? What in the actual fuck? Our heads are about to explode.
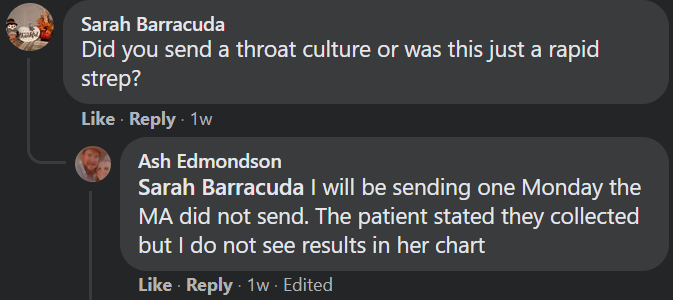
Either this brilliant midlevel NP has discovered the world's first multi-drug-resistant strain of group A streptococcus, or maybe...just maybe...it's not strep! Did our lovely NP check a strep culture (you know, that gold diagnostic standard for strep pharyngitis) before shotgunning at least three different antibiotics? Of course not, because that would make too much sense.
The fact that this mindless NP is posting her clinical conundrum online in a public Facebook group for the whole world to see - and in a such a panicked manner ("Okay I need HELP!!!") - speaks volumes about one of the key skills (or lack thereof) that differentiates physicians from mindless midlevels: the ability to formulate a coherent differential diagnosis. Has FNP Edmondson considered, perhaps, that many other entities and conditions could cause a sore throat? Like, a virus? Mononucleosis? Allergies? Postnasal drip? Fucking hell, a half-assed WebMD search could literally provide a better differential diagnosis than most midlevels. Of course, a proper differential diagnosis would actually require some semblance of a physical exam, of which none is mentioned whatsoever. What did the throat look like? Is it erythematous? Is there an abscess present? Is there cervical lymphadenopathy? Hell, we don't even know how the patient was originally diagnosed with "strep". We, the physician authors here at MidlevelWTF could go on and on until we turn red from scarlet fever. We hear that malpractice attorneys love it too when midlevels publicly flaunt their complete lack of clinical competence while openly broadcasting their medical mismanagement of a patient.
So, as to answer FNP Edmondson's question of "what should I do as next step for this patient?????" How about get off Facebook and consult an actual fucking doctor. And no, we don't mean a DNP.



