New urgent care NP urgently needs some self-awareness
💬 0 comments
Who wants to take bets on how long this oblivious NP will last?
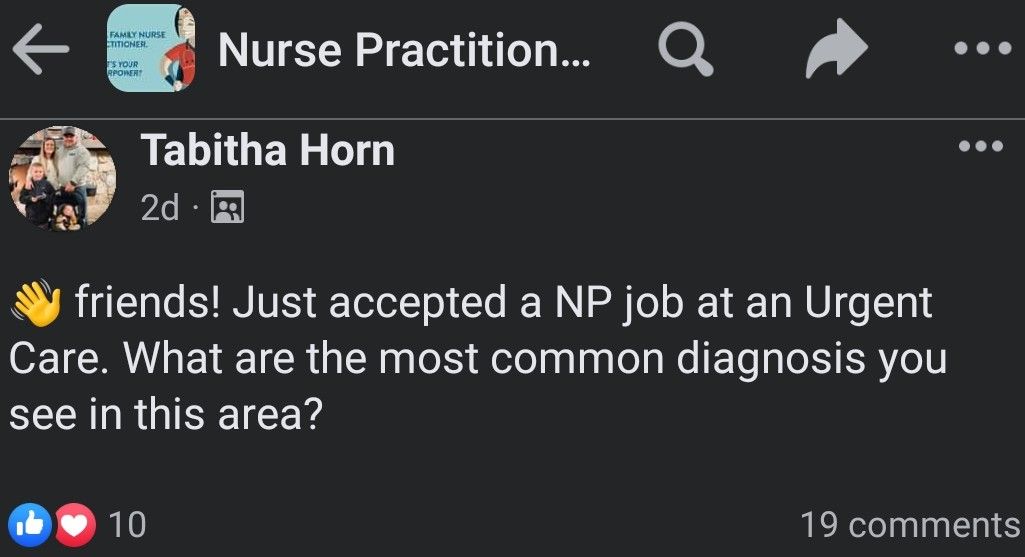
Can you imagine a newly hired surgeon not knowing what kinds of surgeries he/she will be doing? An airline pilot taking a job without knowing what kind of airplanes he/she will be flying? An auto mechanic not knowing what kinds of cars he'll be fixing? No? Well, neither can we. But if Facebook posts like the one above from a group called "Nurse Practitioner Newbies" are any indication, midlevel nurse practitioners seem to take jobs with a blithe disregard for the knowledge base and competencies required for said job. Of course, the employers responsible for hiring these warm bodies straight from the midlevel diploma mills without checking for much more than a pulse are also to blame. But in any case, it's the hapless urgent care patients who will suffer at the hands of a greener-than-spinach midlevel who doesn't seem to have any idea whatsoever why patients usually go to urgent care. Seriously, this is a question so basic that it could be answered by a well-informed layperson possessing a few ounces of common sense, if not the ability to conduct a 5-second Google search.
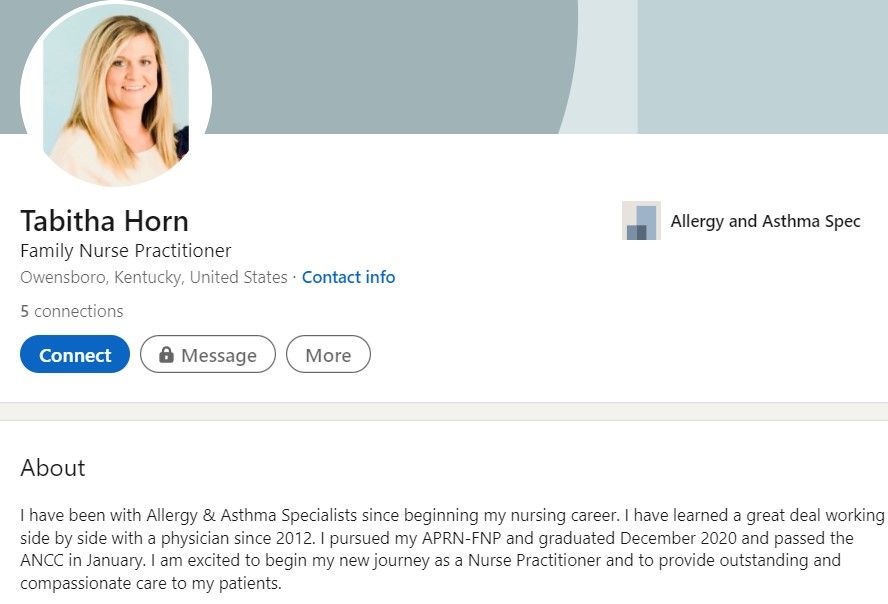
Indeed, it's quite concerning that a family nurse practitioner is posting such a fundamental and common-sense question in a public Facebook group. Naturally, this leads us to question if NP Horn even has the necessary procedural competencies to work in an urgent care. If she doesn't have any awareness of what diagnoses are most common in the urgent care setting, how can we trust that she is capable of performing basic UC procedures such as laceration repairs, abscess I&Ds, applying splints, and administering local anesthesia, to name a few? Given that this newly minted midlevel appears to have spent most of their previous career working in an allergist's office, we would be highly concerned.
By the time we got around to writing this article, the original post has already been featured on various social media venues, resulting in, unsurprisingly, overwhelmingly amounts negative commentary and criticism, especially in physician circles. Ironically, the response in midlevel NP groups to this whole screenshotting affair has been quite the opposite - instead of focusing on the inherently problematic nature of an NP taking an urgent care job seemingly without any idea of what it entails, an army of midlevel minions have been quick to jump to her defense:
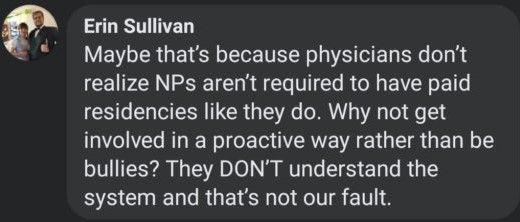
Tsk tsk, Erin. We realize perfectly that NPs aren't required to have paid residencies, and we (at least here at MidlevelWTF) understand the shitshow of a system that is NP education perfectly. It doesn't take a genius MD/PhD to understand that the end product of an online diploma mill with no admission standards other than a thready pulse and clinical "training" consisting of a few hundred hours of shadowing another midlevel is going to be utter dogshit. As the old saying goes, "garbage in, garbage out." The issue isn't whether or not midlevels are required to do a residency. If the educational foundation for NP programs possessed even a modicum of adequacy, we wouldn't be seeing absurdly stupid and embarrassing clinical questions like this being blasted all over social media for the whole word to see and laugh at.
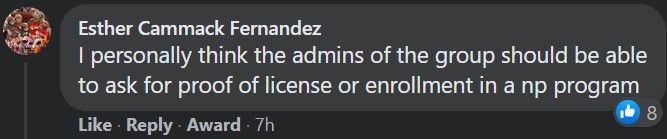
Good luck with that, Esther! Trying to find a needle in a 20,000+ needle haystack should be quite the challenge. And don't forget about all the midlevels who secretly agree with us and are more than happy to act as moles for the cause!
Ah yes, the tried-and-true defense mechanisms of deflection and responding with an ad hominem attack. What better hobby than collecting examples of midlevel incompetence and sharing them with your friends?
What do they call a medical student who graduates at the bottom of the class? Doctor. News flash, Jenn: even the lowest-achieving medical school graduate will have had to pass the USMLE/COMLEX board exams. Need we remind you that so-called doctorally-prepared DNPs got wrecked when they tried taking a watered-down version of the USMLE Step 3? And yet, these failures want to be called "Doctor". There's no "doctor God complex" at play here, Jenn. But if that's what you want to call it when we ask that midlevels have a basic sense of self-awareness and semblance of clinical competency, be our guest!



