"Fairly new" PMHNP wants to know if her "scary med changes" are OK
💬 0 comments
Narrator: This is *not* OK.
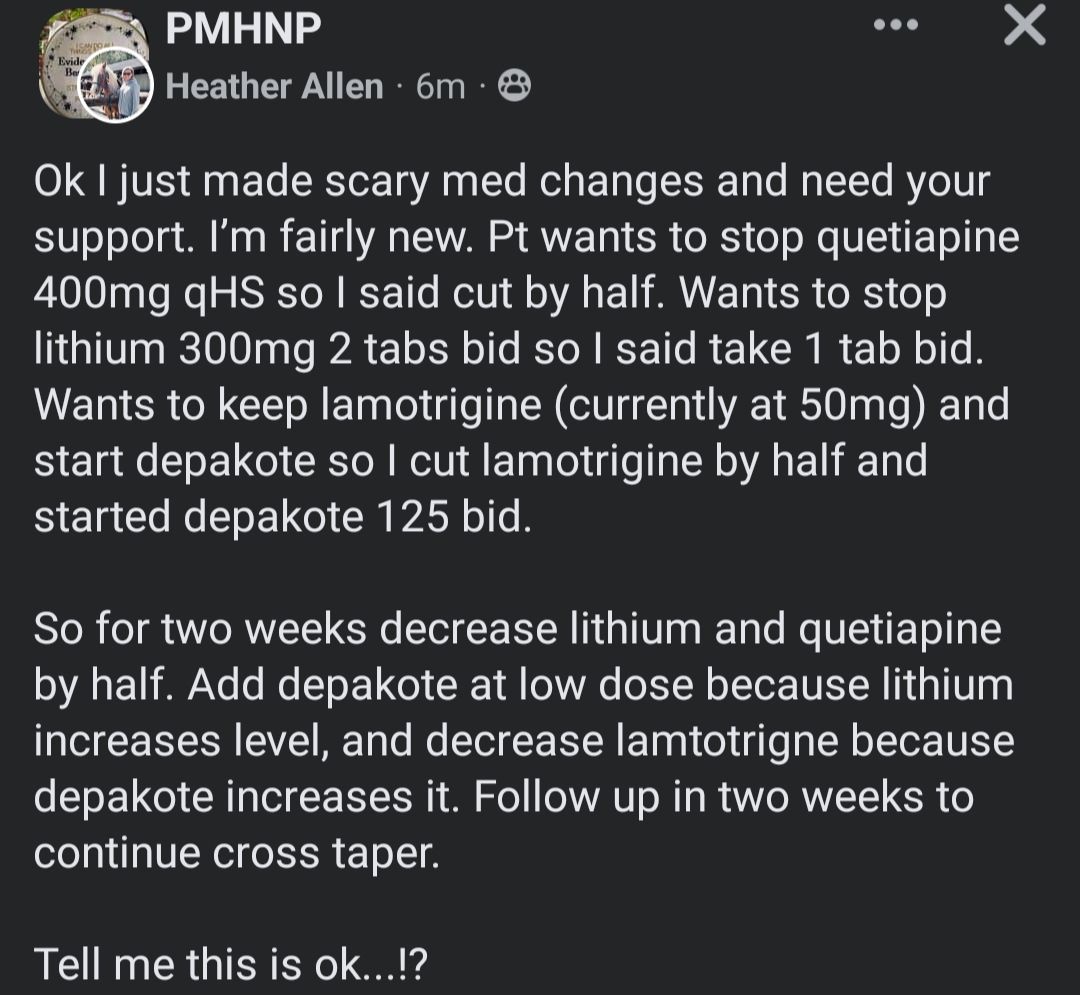
As a patient, it must be really nice to have a clueless midlevel essentially acting as your own personal pharmacy and medication dispenser. Want to just randomly stop taking a medication or two? Sure! Think it would be cool to try taking this new drug? Why the hell not? Depakote Sprinkles sound pretty tasty, after all! It seems like this "fairly new" nurse practitioner by the name of Heather Allen is getting her buttons pushed harder than a vending machine in an ER waiting room. When you're a patient with bipolar disorder/depression dictating your own changes to multiple psychotropic, mood-stabilizing drugs with significant side effects such as lithium, quetiapine (Seroquel), lamotrigine (Lamictal), and Depakote, what could possibly go wrong?
Imagine if a medical student or resident tried to start off a patient presentation to the attending physician by jumping directly to the treatment plan/medication changes without even bothering to mention basic details such as the patient's age, medical history, and current diagnoses. Now imagine if said medical or resident tried to justify their rationale for starting/stopping multiple medications simply because "the patient wanted it". Without a doubt, they would get their ass reamed six ways from Sunday! Indeed, we always find it sadly ironic when lay patients who are tricked into receiving care from moronic midlevels say things like "But the nurse practitioner actually listens and spends more time with me!" As the example above clearly shows, "listening to the patient" and doing whatever the fuck they want with no questions asked is no substitute for actual medical competence. It is certainly no substitute for the rigor of four years of medical school followed by four years of psychiatry residency!
Admittedly, NP Heather deserves some credit, at least, for realizing that her medication changes are "scary". Indeed, some of the attending psychiatrists who saw this Facebook post were absolutely mortified. One described it as "Russian roulette with meds". Assuming the patient in this scenario has bipolar disorder, "Russian roulette" is a pretty damn accurate way of describing PMHNP Heather's decision to suddenly discontinue/taper the gold-standard medications lithium and quetiapine. Another physician snarkily replied, "What else does the patient want to do? Commit suicide? Here is the rope!"
Increased suicide risk aside, the sudden discontinuation of lithium along with an antipsychotic drug like quetiapine raises serious concern for adverse effects, such as precipitation of the very episodes this regimen is intended to treat. Specifically in the case of lithium, PMHNP Heather's decision to halve the patient's dose of lithium in only two weeks is questionable at best, given that most medical literature recommends a taper of four weeks at a minimum, and preferably three to six months. One psychiatrist described PMHNP Heather's medication adjustments as "a straight shot into a manic episode", while another non-psychiatry physician remarked, "even I know that's a disaster of a plan".
One of our colleagues then pointed out the obvious futility of trying to tease apart the individual effect of each medication change at future follow-up visits. Indeed, this PMHNP appears to have committed one of the cardinal sins of medicine and medication management: unless you have a damn good reason (which is seldom the case for midlevels), don't make multiple changes to multiple medications at the same time!
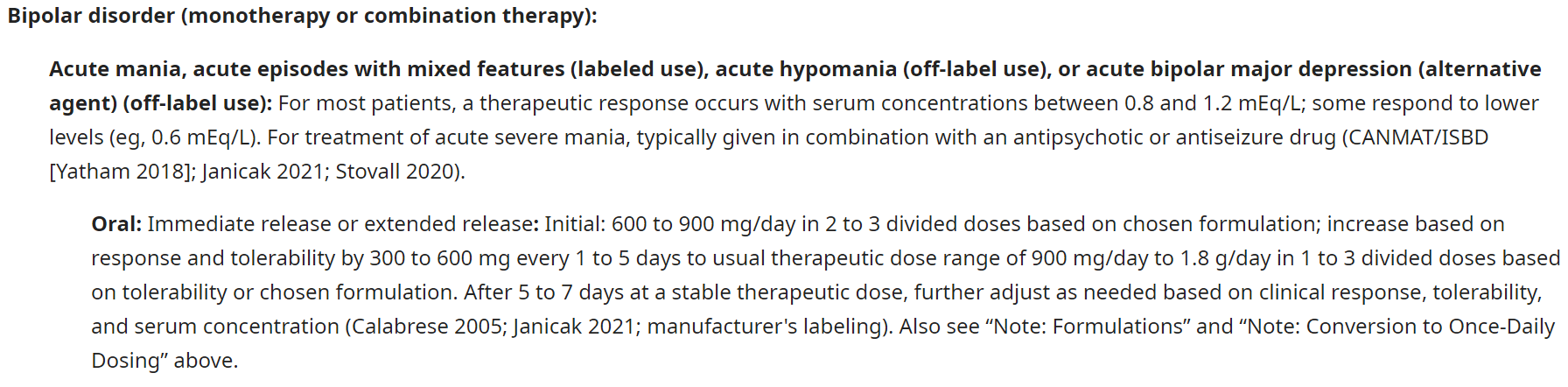
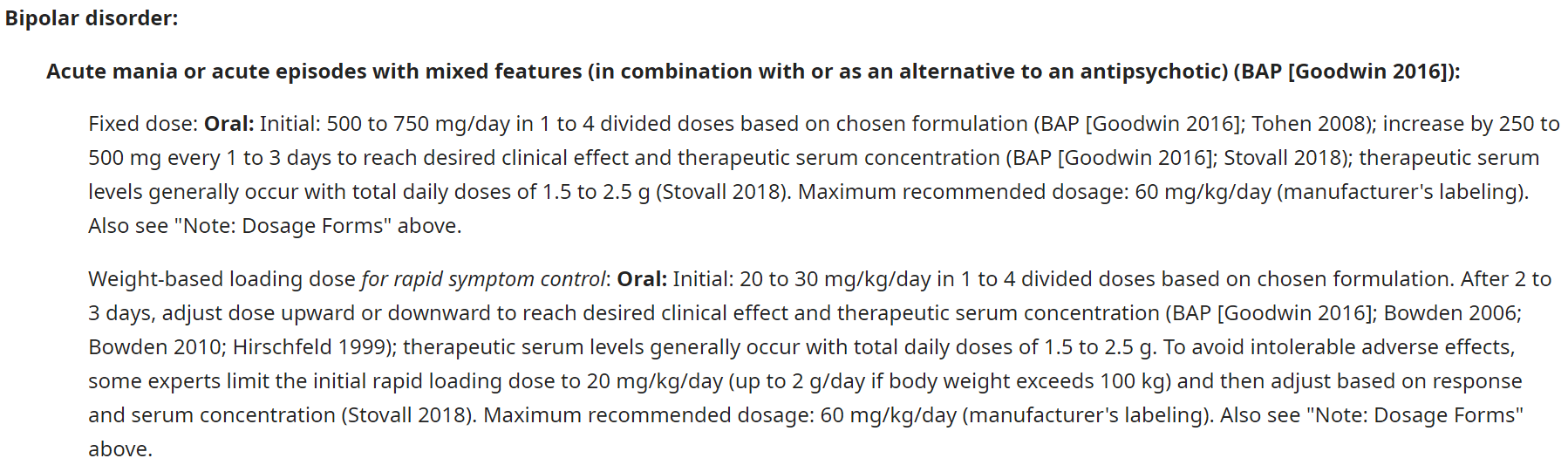
But wait, there's more! If we take a deeper dive into pharmacology (which is apparently not taught in nurse practitioner school), there are even more midlevel what-the-fucks to be had. For one, this patient's original lithium dosing of 300 mg BID (twice a day) is well below the usual therapeutic window of 900-1,800 mg/day. Setting aside the question of why we're swapping mood-stabilizing medications for no apparent reason whatsoever, one can also appreciate that PMHNP Heather's decision to start Depakote at the laughably low dose of 125 mg BID is analogous to pissing in the wind when the usual starting dose is 500-750 mg/day and the therapeutic window is typically between 1,500-2,500 mg/day.

Also, where the hell did she get the idea that lithium increases Depakote levels? Lithium is not metabolized by the body, not protein-bound, and almost entirely renally excreted to the tune of 95%. By contrast, Depakote (valproate/sodium valproate) is primarily metabolized in the liver, with <3% being excreted unchanged in urine. Had she bothered to attend an actual medical school-caliber pharmacology class, perhaps she would have appreciated these basic concepts of drug metabolism.
So, in short, if we were to answer PMHNP Heather's question if this is "OK", the answer would be a resounding no, it is certainly not fucking okay at all. For her own sake, we can only hope that Heather advised her patient about the very real risks of the "scary med changes" she has made. If not, well...we're sure that medical malpractice attorneys always appreciate it when the defendant has already dug his/her own grave in the form of a public Facebook post!



