Brilliant questions from Kahlil Demonbreun, DNP, RNC-OB, WHNP-BC, ANP-BC, FAANP, FAAN
💬 0 comments
Not so brilliant after all.
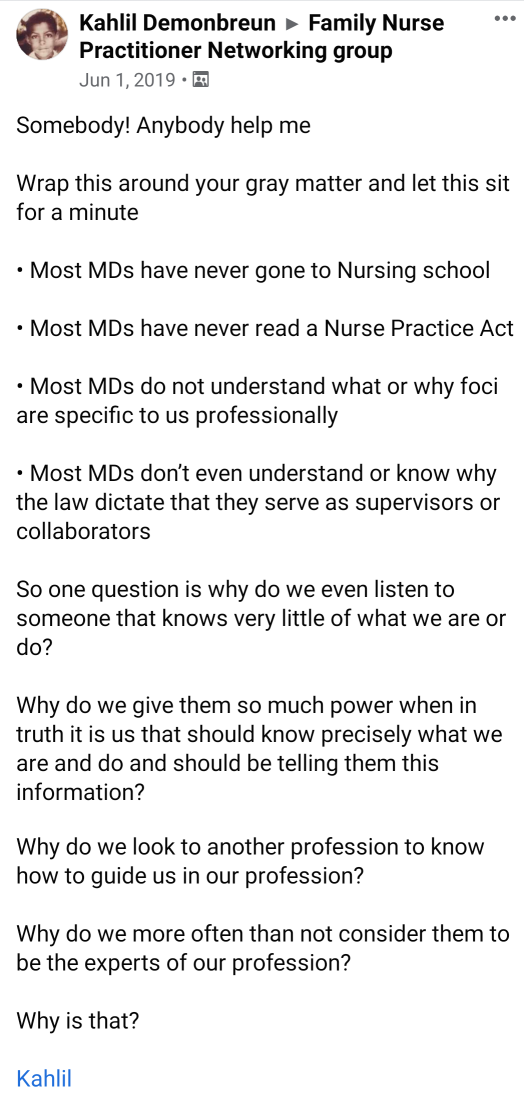
We recently came across this gem of a post by Kahlil Demonbreun, DNP, RNC-OB, WHNP-BC, ANP-BC, FAANP, FAAN (geez, don't you hate it when they lay out all of their silly credentials like that?) who is apparently the AANP state rep for South Carolina, as well as the "Women's Health Medical Director" for the Columbia VA Health Care System. Don't you think it would be reasonable for, you know, a physician to be the medical director, and not a midlevel? Not at the VA, because our veterans deserve the best! But I digress. Let's return to our original topic, Kahlil's list of truly thought-provoking points, and respond to them one by one!
- Most MDs have never gone to nursing school
- No fucking shit, Kahlil. That's because we decided to go to medical school instead.
- Most MDs have never read a Nurse Practice Act
- Why would we? We're physicians, not nurses. But just for fun, we decided to go and read some. For example, California's NPA states that the practice of nursing includes "direct and indirect patient care services that ensure the safety, comfort, personal hygiene, and protection of patients; and the performance of disease prevention and restorative measures." Do nurse practitioners suddenly stop doing this once they become an NP? Based on the rest of the content featured on MidlevelWTF, we'd say so!
- Most MDs do not understand what or why foci are specific to us professionally
- What the hell are foci? Is it one of those useless nursing theory things you learn as part of a 100% online DNP degree? Sorry, not interested. I'd rather stick to the evidence-based medicine I learned at my brick-and-mortar medical school.
- Most MDs don't even understand or know why the law dictate that they serve as supervisors or collaborators
- Wow, ballsy statement there, buddy. Let's make one thing very clear here: physicians know exactly why they have to supervise and collaborate with nurse practitioners. It's because we don't want NPs to consult random, unvetted people on Facebook and end up accidentally killing patients. It's because we want a fully trained expert around to make sure the midlevel knows what the fuck they're doing.
- ...Why do we even listen to someone that knows very little of what we are or what we do?
- See above. As physicians we may not know how to be a nurse, but when you become a nurse practitioner to diagnose/treat patients and/or perform procedures, you practice medicine, and by definition that is something we know a lot about.
- Why do we give them so much power when in truth it is us that should know precisely what we are and and do and should be telling them this information?
- Know your roots, Kahlil. You want to be precise? Don't forget that the first NP program was created in partnership with a physician.
- Why do we look to another profession to know how to guide us in our profession?
- See above. If you want to practice medicine without a guide, then become a physician, not a midlevel nurse practitioner. Until then, as with every other line of work, get used to the idea that people with more training and experience supervise people with less training and experience.
- Why do we more often than not consider them to be the experts of our profession?
- Again, see above for the answer to this redundant question. If you want to be an expert in medicine, be a physician!



