Puzzled nurse practitioner consults Facebook for a patient with critical hyperkalemia
💬 0 comments
It's anyone's guess whether the patient in question is dead or alive.
Virtually any physician would shit their pants after seeing their patient's lab results come back with a dangerously high potassium level of 9.6. After all, any second-year medical student would know that critical electrolyte abnormalities such as hyperkalemia warrant emergent treatment. And while we physicians may be shitting our pants initially, thanks to our extensive knowledge, training, and experience - particularly those of us who practice as hospitalists, nephrologists, emergency physicians, or critical care/ICU specialists - we also know how to quickly evaluate and manage patients with severe, life-threatening electrolyte derangements while our pants are soiled. Unfortunately, the same cannot be said of the dumb-as-fuck nurse practitioner who wrote this now-deleted anonymous post on Facebook - clearly, their reaction is more akin to a deer caught in a pair of very bright headlights. Indeed, it's too bad that they decided to post anonymously, because otherwise, we would have enthusiastically administered a thorough public humiliation and roasting of their stunning lack of medical knowledge. Just as well, because as physicians like us know, people with severe burns tend to have issues with kidney injury and hyperkalemia. 😂

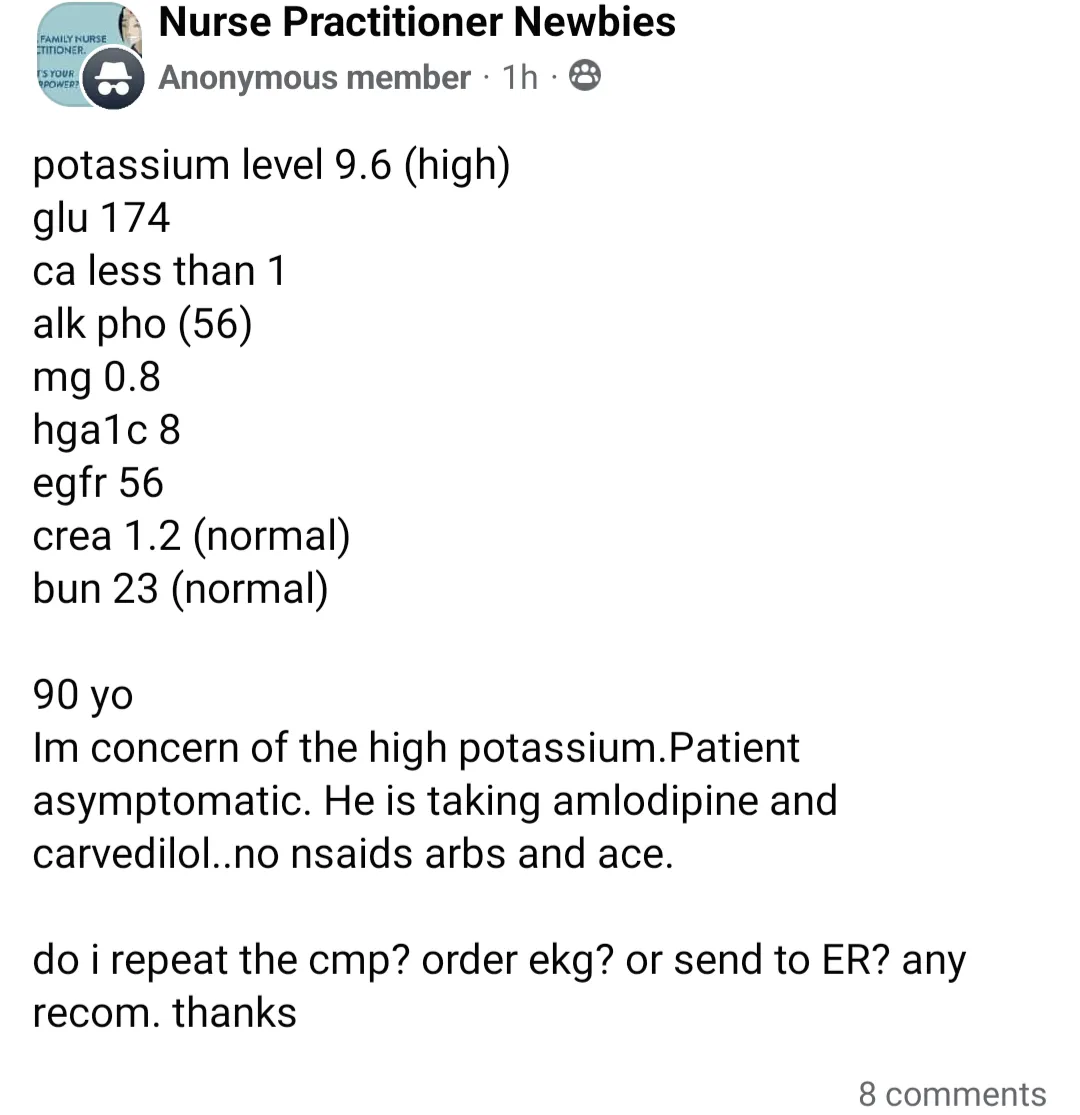
To further dissect this idiot NP's completely illogical medical decision-making and why it makes zero fucking sense, let's delve into the nitty-gritty of hyperkalemia for our layperson readers. With a normal reference range of 3.5 to 5.2 mEq/L for adults, a potassium level of 9.6 isn't just high - it's really fucking high. Sure, maybe the lab report could be inaccurate on the off chance that the lab is having a bad day, but in a 90-year-old patient who likely has diabetes and chronic kidney disease, stage 3 with a hemoglobin A1C of 8 and a GFR of only 56, more likely than not these lab values are accurate, even after accounting for a hemolyzed specimen. In any case, this isn't some borderline-high potassium where you have the time or luxury to "recheck" a BMP/CMP or "order an EKG" - if your potassium level is almost 10, it's more a matter of "YOU NEED TO GO TO THE EMERGENCY ROOM RIGHT FUCKING NOW!" - "HOW ARE YOU STILL ALIVE?!" - "WHAT'S YOUR CODE STATUS BECAUSE YOU COULD DIE ANY FUCKING SECOND?!" You might think we're exaggerating, but we're not, because a potassium level over 7, and certainly anything over than 9, predisposes the patient to a wide variety of highly unpleasant cardiac arrythmias such as ventricular fibrillation, pulseless electrical activity (PEA), and asystole, which, to put it mildly, are all incompatible with life. The majority of ER docs would be throwing the entire kitchen sink at this patient, including insulin/dextrose, calcium gluconate or calcium chloride, high-dose albuterol, and maybe Lokelma/Kayexalate. They might even be hammer-paging the nephrologist on call to inquire about the necessity of emergent hemodialysis. (Remember your AEIOUs from medical school?) On the other hand, if you're a midlevel NP whose IQ is equivalent to a pile of bricks and your plan is to fuck around and find out by posting on Facebook and waiting for an EKG to see if your critically hyperkalemic patient has any EKG changes such as peaked T waves, QRS widening, P wave flattening, or heart blocks, chances are your patient has already died from cardiac arrest. Not that it really matters - we've yet to meet a midlevel nurse practitioner that can competently interpret an EKG.
ACLS refresher: Asystole is not a shockable rhythm!



