Idiot NP can't make the diagnosis when it's staring her in the face
💬 0 comments
This picture is worth nowhere near a thousand words.

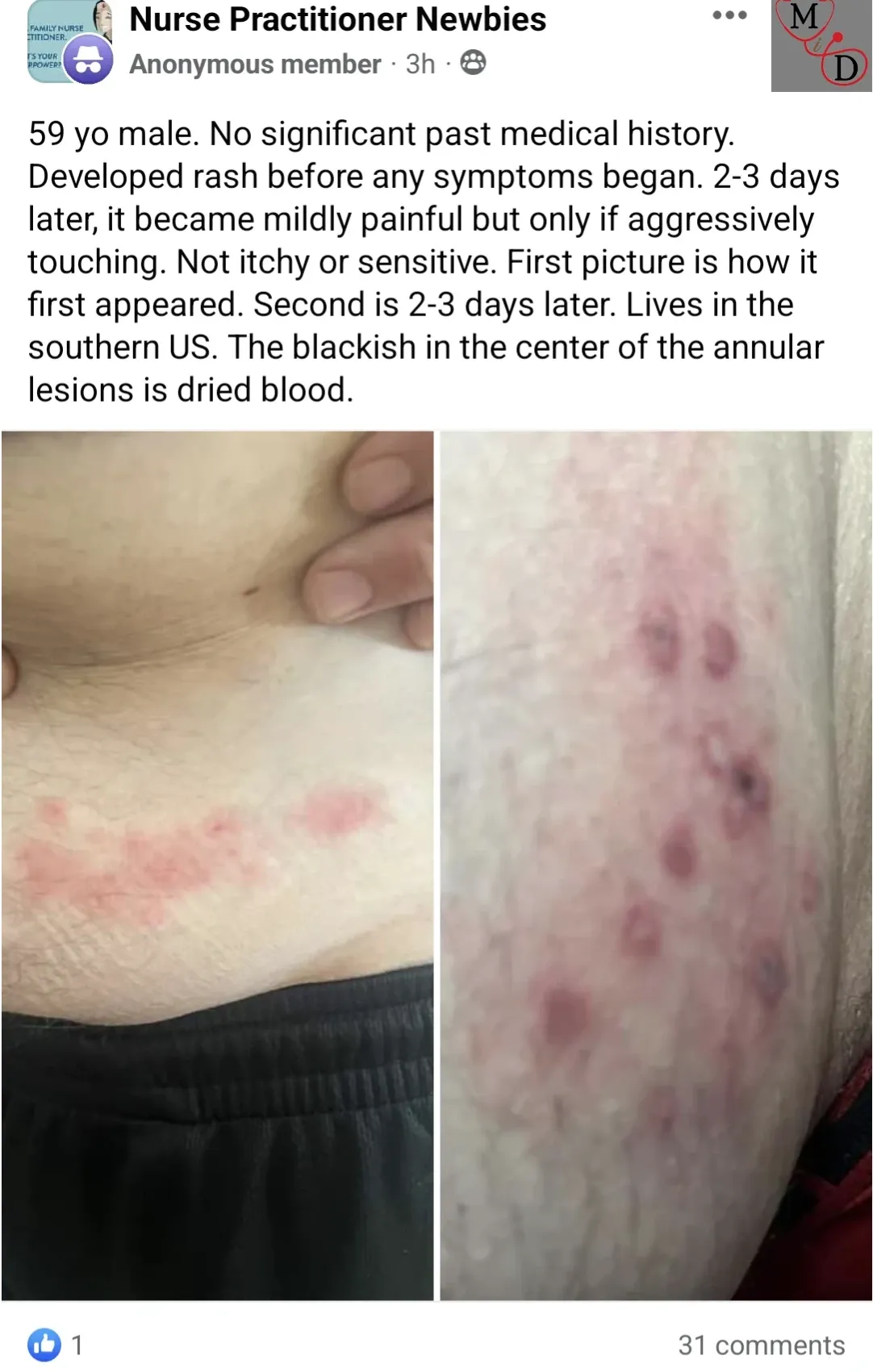
As the old saying goes, "A picture is worth a thousand words." In this case, though, it's really worth just one - the name of the viral disease most likely to be causing the condition pictured here - shingles. One is probably also an accurate count of the number of brain cells possessed by the midlevel nurse practitioner who took the time to take these lovely textbook pictures of the dermatomal rash on her male patient's abdomen and post them on Facebook for countless eyeballs to see, instead of utilizing an appropriate clinical reference or textbook or consulting a more experienced colleague.
Just like the varicella zoster virus (VZV) that causes chickenpox during childhood and shingles in adults, word tends to spread quickly among physician circles about just how fucking stupid you are. And we wonder about the "no significant past medical history" - did this midlevel NP ever ask the patient if he had chickenpox as a child? Based on the level of stupidity we've established, we'd wager to guess that the answer is no. With a birth year of 1963 or 1964 for this patient, this would actually be fucking important to know, because it wasn't until 1995 that the varicella vaccine was added to the childhood immunization schedule in the United States.
This Facebook post is also a perfect example of why its highly inadvisable to consult social media for medical advice, as evidenced by the very "helpful" suggestions made below by other clueless midlevel nurse practitioners.
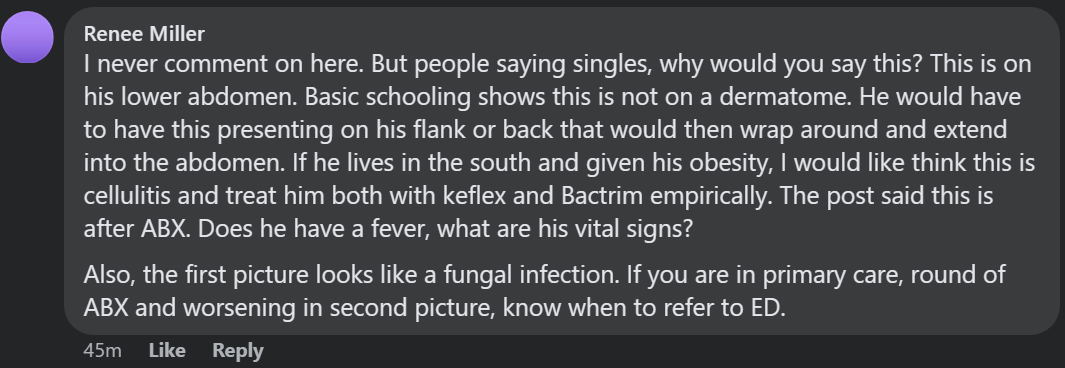
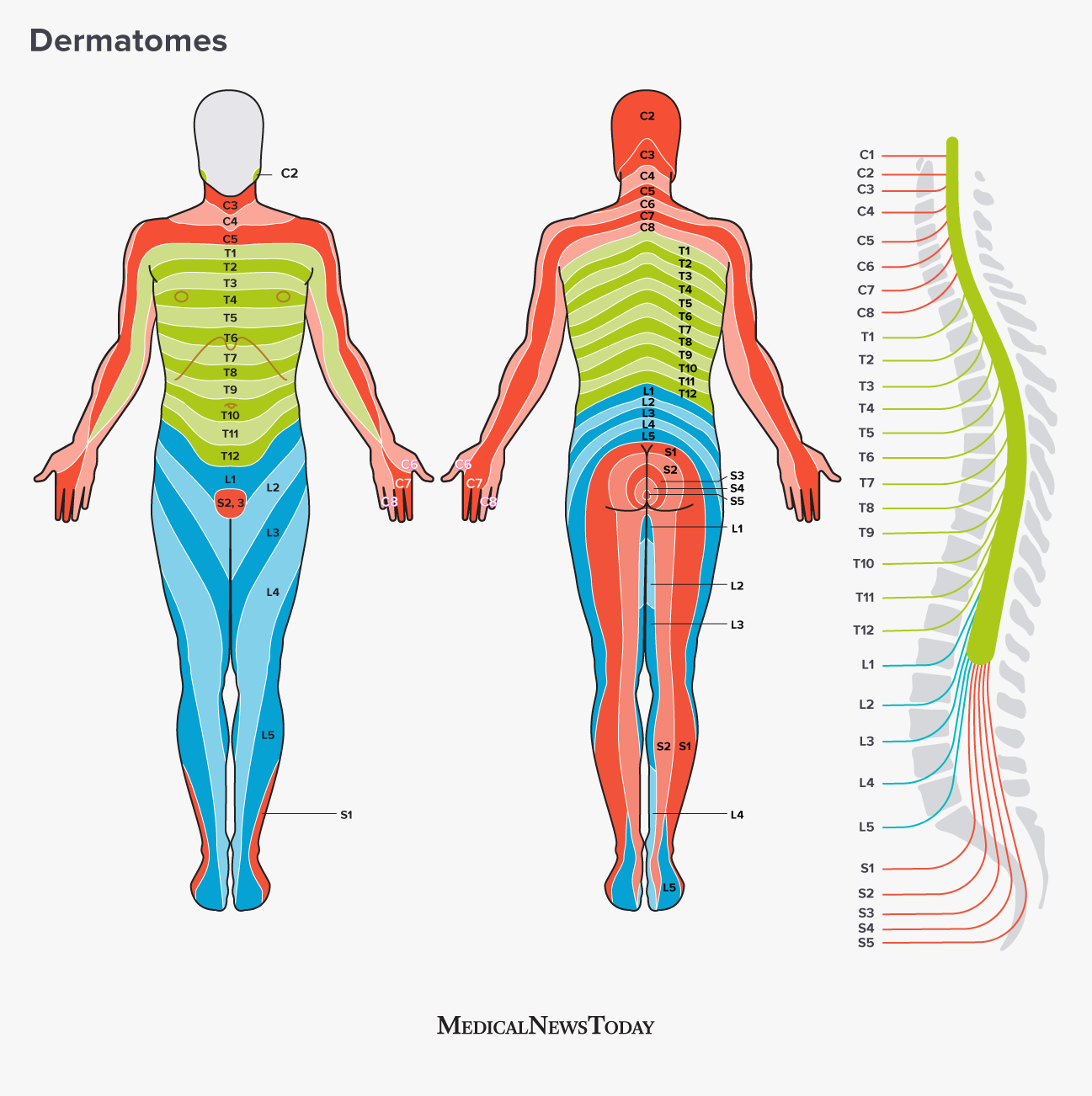
Here, we have a very severe case of Dunning–Krugerism. This midlevel nurse practitioner is extremely confident that it cannot be "singles" because "this is not on a dermatome", thanks to her "basic schooling". Evidently, she has never seen a case of shingles on the anterior abdomen, instead throwing up a differential diagnosis of cellulitis or fungal infection. We have serious doubts as to whether or not Ms. Miller has seen either of those two pathologies.
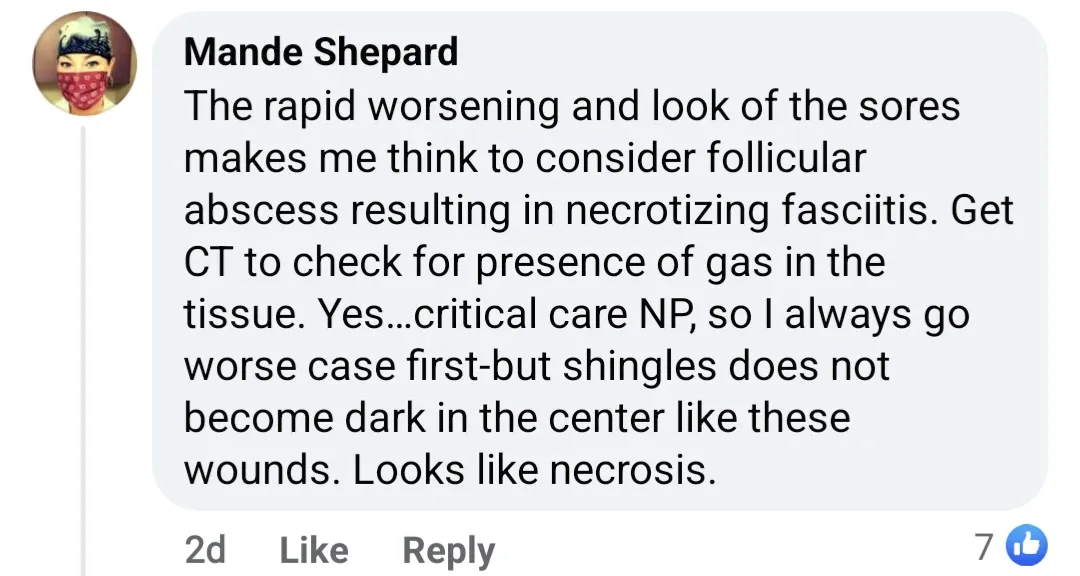
Necrotizing fasciitis? What the fuck? If this were truly a case of necrotizing fasciitis (which can spread rapidly within hours), the patient would quite likely be dead by the time the first NP ordered a CT scan "to check for presence of gas in the tissue". It goes without saying that if there was true concern for necrotizing fasciitis, the next stop would be the operating room STAT, not dicking around with imaging and further delaying definitive diagnosis and management. And if you really want to be pedantic, it's important to know that not all organisms responsible for necrotizing fasciitis are gas-producing. One would think that a person who's supposedly a "critical care NP" would be fully aware of this, but evidently not!
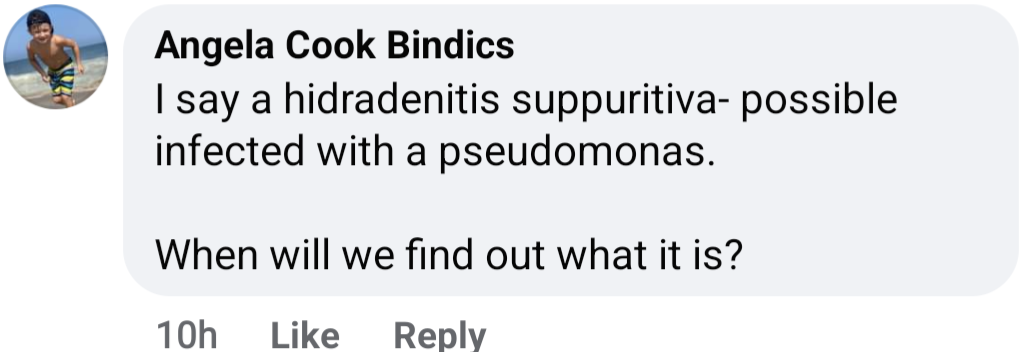
The timeline, location, and distribution of the pictured lesion is not consistent with hidradenitis suppurativa. And what the fuck, where are we getting Pseudomonas from? Did she just randomly make that up out of thin air?
Finally, we have the bug bite crew chiming in with the immensely helpful differential diagnoses of sand flea bites and spider bites from a brown recluse. Needless to say, anyone with an ounce of clinical experience (i.e. an actual physician, not a midlevel) and anyone who has actually been bitten by any of these critters would be able to confidently state why these ideas don't make any fucking sense at all.



