By all means, try intubating a preemie 11 times
💬 0 comments
Sadly, the proliferation of incompetent midlevels in neonatal ICUs, particularly neonatal nurse practitioners, is all too common these days.
Originally posted on Reddit. Transcribed and lightly edited for grammar and clarity.
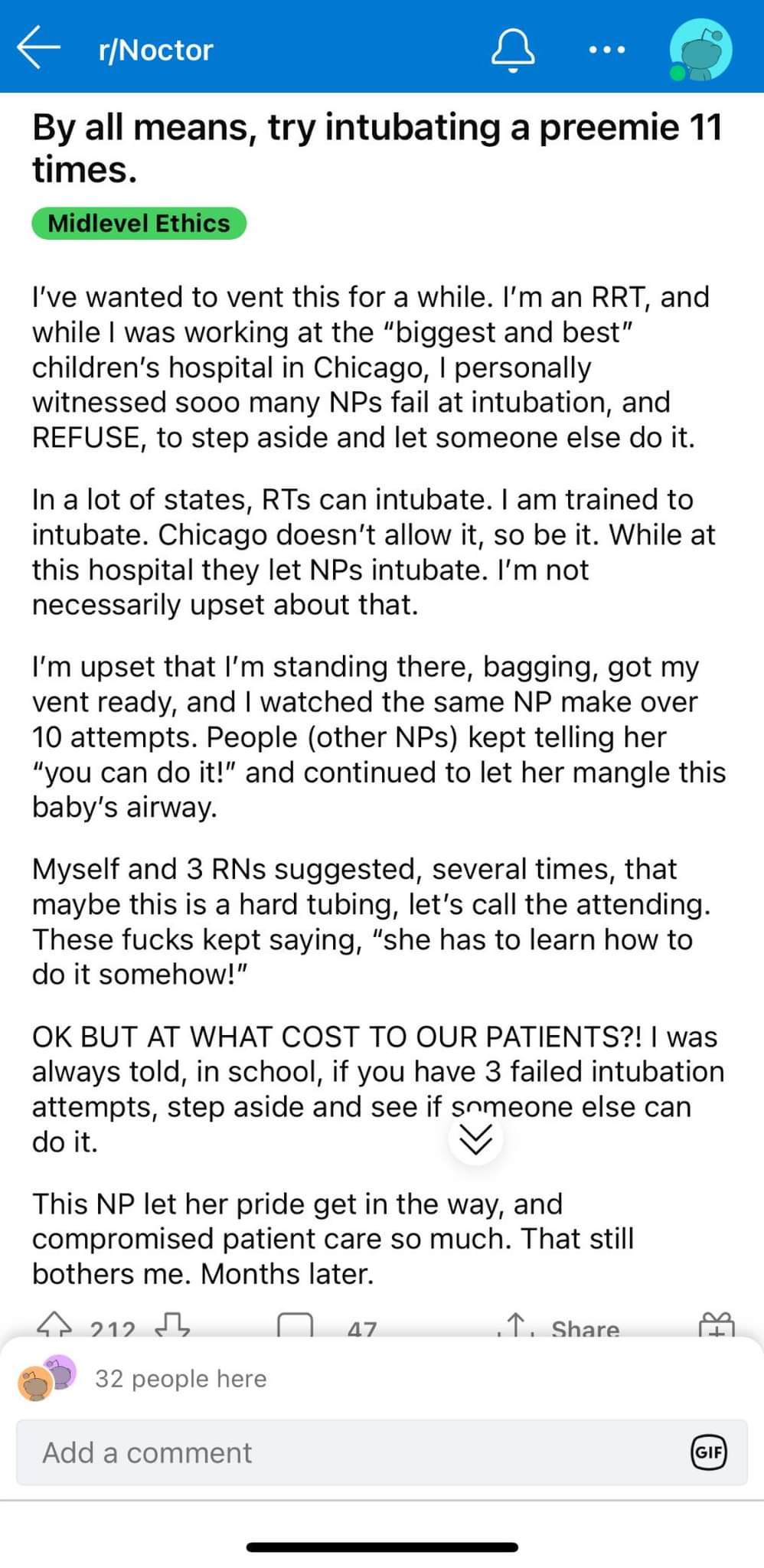
I've wanted to vent this for a while. I'm an RRT (registered respiratory therapist), and while I was working at the "biggest and best" children's hospital in Chicago (editor's note: likely Lurie Children's Hospital at Northwestern), I personally witnessed soooo many NPs fail at intubation and REFUSE to step aside in order to let someone else do it.
In a lot of states, RTs can intubate. I am trained to intubate. Chicago doesn't allow it, so be it. While at this hospital they let NPs intubate. I'm not necessarily upset about that.
I'm upset that I'm standing there, bagging, with my ventilator ready, while watching the same NP make over 10 attempts. People (other NPs) kept telling her
"You can do it!" and continued to let her mangle this baby's airway.
I and 3 RNs suggested, several times, that maybe this is a hard intubation - let's call the attending physician. These fucks kept saying, "She has to learn how to
do it somehow!"
OK, BUT AT WHAT COST TO OUR PATIENTS?! I was always told in school that if you have three failed intubation attempts, you should step aside and see if someone else can do it. This NP let her pride get in the way, and compromised patient care so much. That still bothers me, months later.
Additional Commentary by Midlevel.WTF
Per one of our contributors in the field of emergency medicine, it is standard practice in residency to be allowed only a couple of attempts at intubation before deferring to a more senior colleague (e.g. the attending physician). Certainly, allowing a single person to attempt (and fail) intubation 10-11 times is fucking unheard of and downright dangerous to the patient, given the high risk of iatrogenic airway trauma from multiple failed intubations. We don't have enough information to speculate on what exactly happened here, but clearly, something had to be way fucking wrong with the midlevel nurse practitioner's intubation skills and/or technique. After a couple of attempts, it's time to swallow your damn fucking pride and allow someone who actually knows what they're doing, specifically how to safely and competently intubate a tiny-ass premature infant - e.g. a pediatric intensivist physician who actually want to fucking medical school and earned a medical degree, completed pediatrics residency, and took the extra step of spending even more years of their life underpaid in order to do a pediatric critical care fellowship. All in all, that adds up to a decade (or more) of medical training.
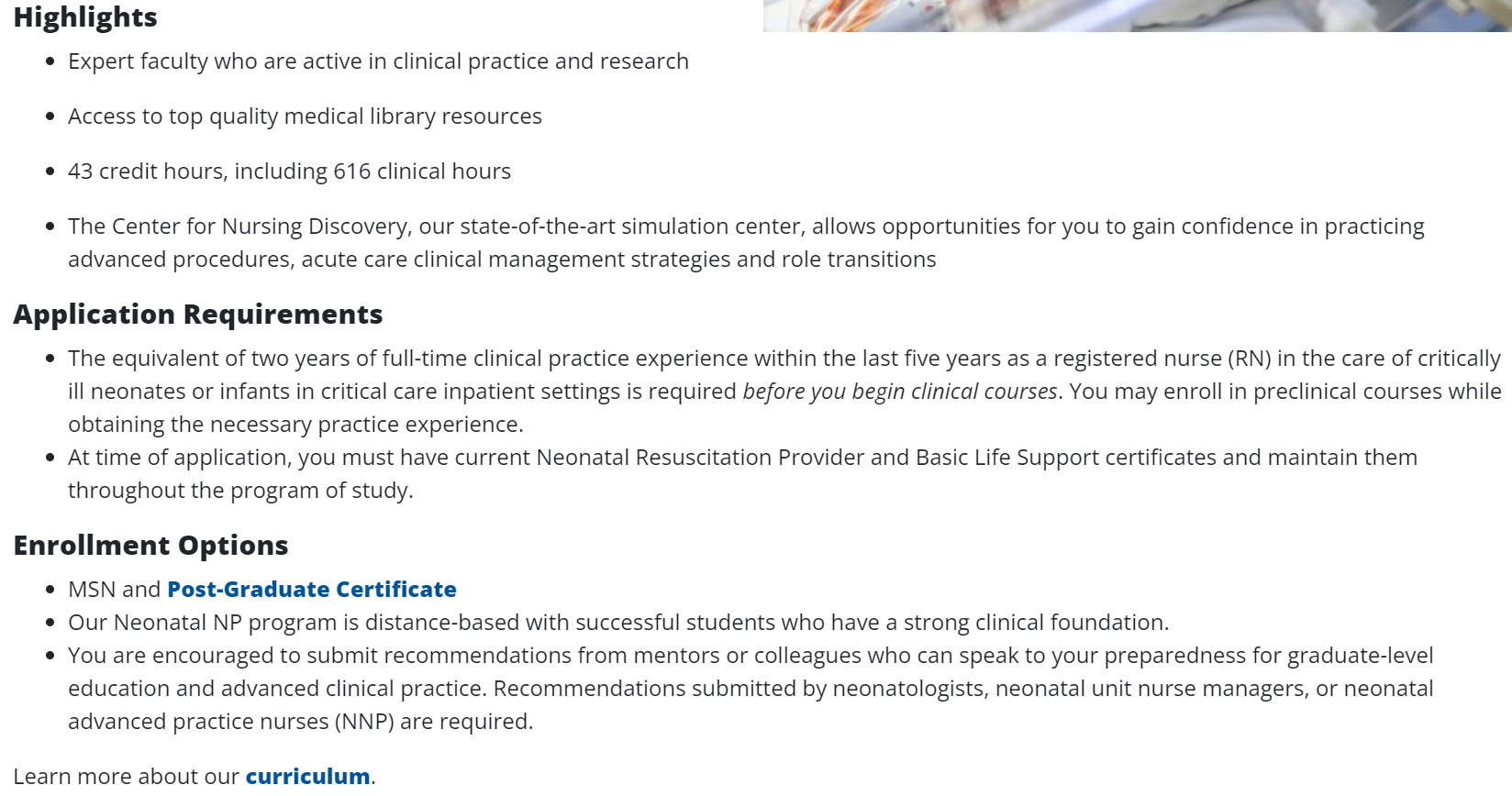
Meanwhile, the training required to become a neonatal nurse practitioner is a sad fucking excuse of a joke compared to that of a pediatric NICU/PICU physician. It's like comparing a worker at McDonald's to Gordon Ramsay - and no offense to the people who work at McDonald's. Imagine being "qualified" to intubate a critically ill neonate with only 616 hours of training. It doesn't take a Benjamin Spock-level IQ to realize that 600+ hours is not anywhere near sufficient for someone to become proficient in the fine art of intubation, especially in emergent settings where the airway needs to be rapidly secured.
 Sin Young Kim
Sin Young Kim Maria L Buis
Maria L BuisIn fact, several studies report a bare minimum of 50-200 successful endotracheal intubations to achieve a reasonable level of proficiency and competency. While this is certainly a realistic and achievable goal for physicians by the time they complete residency or a critical care fellowship, it's certainly difficult, if not impossible to believe that any neonatal nurse practitioner out there would have developed an even remotely comparable level of intubation competency after 600 clinical hours, given the vast amount of other knowledge to be attained in the realm of neonatal/pediatric critical care. And this world of difference, unfortunately, is how we end up with scenarios like the one above in which a midlevel nurse practitioner is so arrogantly incompetent that she takes 11 fucking attempts to intubate a poor baby.



