The chair of the American Board of Internal Medicine is a midlevel simp
💬 0 comments
Gee, I wonder, could there possibly be a difference between a physician versus someone who's not a physician?
Perhaps the only thing worse than a midlevel running amok and harming patients under the guise of full practice authority is a fellow physician and leader that actively simps for them. Enter Yul Ejnes, MD, the current chair of the American Board of Internal Medicine (ABIM) Board of Directors, and his hot mess of a tweet:
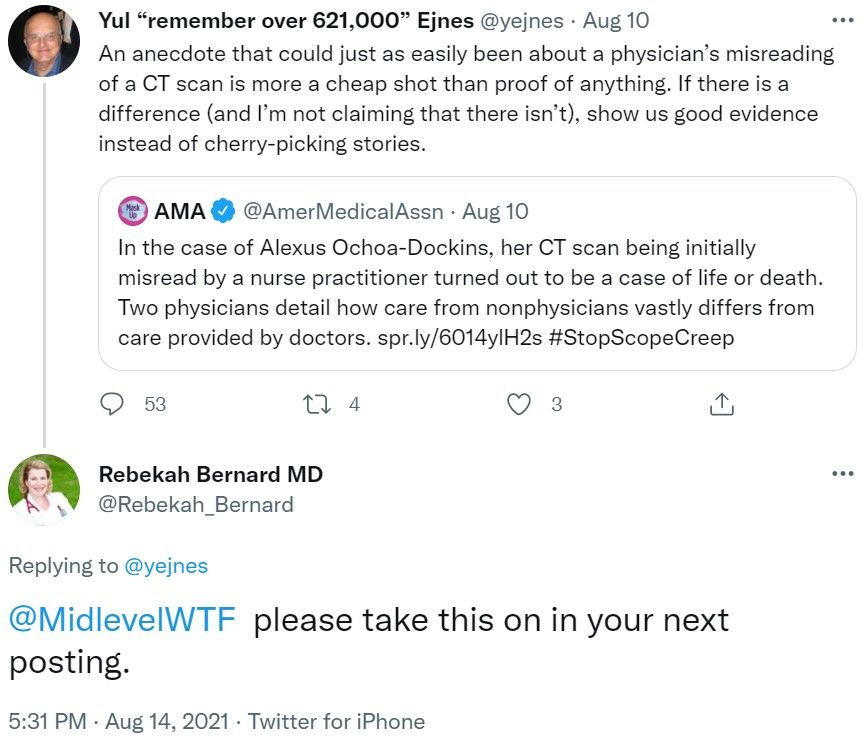
For those not in the know, the case of 19-year-old Alexus Ochoa-Dockins is a watershed example of midlevel malpractice, the sheer inadequacy of nurse practitioner education and clinical training, and the folly of letting midlevel nurse practitioners and physician assistants practice independently without direct physician supervision.
Anyone familiar with the many horrifying details of this case would immediately tell ole' Yul to pull his head out of his ass. The story of Alexus-Ochoa-Dockins' death at the hands of an incompetent nurse practitioner was not merely an anecdote that "could just as easily been about a physician's misreading of a CT scan" - it was a full-blown medical malpractice case involving an NP's chain of errors upon errors that went to jury trial and eventually settled for six million dollars.
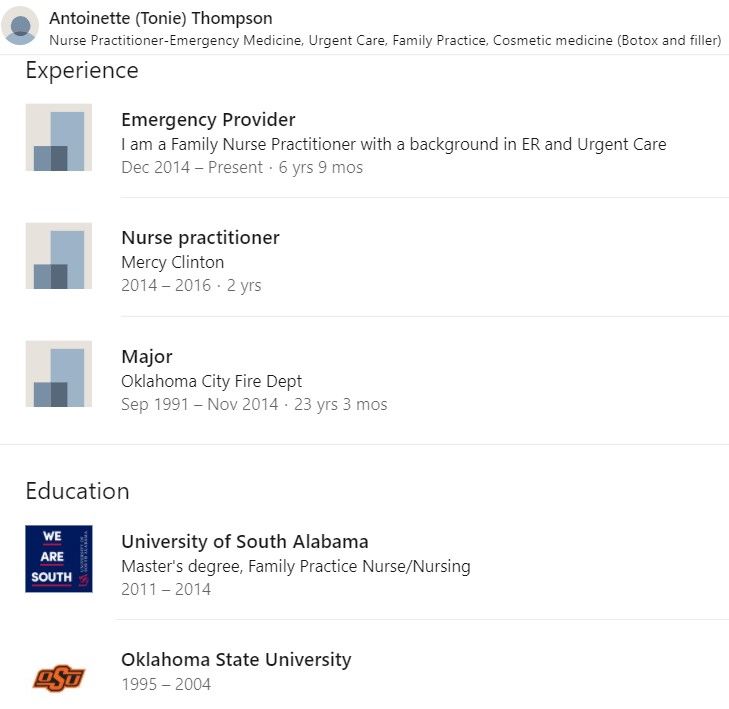
The deposition of the incompetent family nurse practitioner in question, Antoinette Thompson-Ducasse, is particularly damning. Who in the actual fuck would straight-up ignore a paramedic's concern for pulmonary embolism, treat physiologic sinus tachycardia with adenosine, mistake massive bilateral pulmonary emboli on a CT with right heart strain as a "crushed sternum" (???), and start prophylactic-dose anticoagulation in a hemodynamically unstable patient? An FNP practicing independently and out of scope in an emergency department only months after graduating from a mostly-online NP program, that's who!
Simply put, there's no way in hell a physician (and likely even a fourth-year medical student, let alone a seasoned emergency medicine physician) would have failed to recognize or at least entertain the possibility of a pulmonary embolism in a young female who was not only tachycardic, tachypneic, hypoxic, and complaining of chest pain and shortness breath, but also on oral contraceptives. Meanwhile, in the gilded la-la land of his Brown University ivory tower, Dr. Ejnes, chair of the ABIM, thinks this case is "more a cheap shot than proof of anything" and, amazingly, has the gall to ask "if there is a difference" between physician and non-physician care. If Dr. Ejnes really thinks that a physician could have "just as easily" made the same mistakes as the aforementioned NP, perhaps that's more a reflection of his own aptitude, or lack thereof, for the practice medicine. Shut it down folks - if Dr. Ejnes really thinks that there might not be any difference between physicians and non-physicians, perhaps it's time to start allowing midlevels to take physician specialty board certification exams. Hell, why not allow members of the general public (including those who have "done their research" on the COVID vaccine) to sit for the medical boards? Practicing medicine must be so easy, even an anencephalic baby could do it! One must wonder about the economic and financial motivations for Dr. Ejnes to publicly make such pro-midlevel, anti-physician statements - perhaps the fact that there are no less than 22 nurse practitioners on staff at the medical group that he co-founded in 1995 might have something to do with it?
Keep in mind that ABIM is the governing body in charge of board certification for internal medicine physicians. Say what you want about the ABIM's exorbitant ransoms fees for board certification and its infamous and controversial Maintenance of Certification (MoC) programs, but at least on paper, the ABIM, like every other medical specialty certifying board, is tasked with setting the minimum standard for the required knowledge and training that physicians must have in their specialty. If ole' Yul wants some "good evidence" that there are indeed major differences in the qualifications of physicians versus midlevels, then perhaps he should do more reading, just like we were always told to do as medical students. And what exactly does he consider to be "good evidence"? Is the above comedy of errors not sufficient? Does he want a blinded, randomized controlled trial where the unfortunate patient-subjects have no idea if they're being treated by a physician or a midlevel fresh out of online school with a few hundred hours of clinical "experience"? Does he really want to question the axiom that someone with substantially more knowledge, training, and experience is going to be more competent and make fewer errors than someone with less knowledge, training, and experience? Sorry, Yul. There's no cherry-picking here - as documented on MidlevelWTF and elsewhere, countless examples of midlevel incompetence exist. What you regard as an "anecdote" is someone else's loved one, friend, or family member killed at the hands of an incompetent midlevel pretending to be a physician. It doesn't take a needless patient death to see that there's a difference - a big difference - in the quality and safety of care provided by physicians versus non-physician providers.
Are you as upset as we are about Dr. Ejnes' statements?
Call or write to the ABIM: https://www.abim.org/contact/



